Veterinary Advice Online: Rabies Virus.
The information contained within this article covers a range of topics designed to fully educate pet owners about rabies virus in dogs, cats and other domestic and wild animal
species. Topics on vaccination of pets, side effects of rabies vaccines and human health
implications of rabies are also covered. For the Australians among us, information on bat
Lyssavirus (Australian rabies) has also been added. The information presented is detailed (but still easy to understand) because we are aiming to educate owners and the public thoroughly and to provide them with enough information that they might be better informed and able to troubleshoot problems with their own pets. The topics are covered in the following order:
1) What is rabies? - this is a short definition and basic explanation of what rabies is.
2) Which animals are at risk of contracting this virus?
3) Transmission - How do pet animals and humans catch this disease? - this section contains information about where and how animals and people can contract rabies and the environments and occupations that are higher in risk.
4) Symptoms and Signs - What does this virus do to dogs, cats, humans and other animals? This section contains the following subsections:
4a) How do rabies viruses work (how do they replicate and destroy cells etc.)?
4b) How does rabies affect the brain (what neurological symptoms of rabies are seen)?
4c) How does rabies affect the salivary glands (how is rabies spread)?
4d) Rabies vaccine-associated diseases (rabies caused by vaccines).
5) Testing and Diagnosis. This section contains the following subsections:
5a) Obtaining a sample to test - includes sections on euthanasia of rabid animals; how to capture and
confine a rabid animal; how to store deceased animals prior to sending them to the lab.
5b) The fluorescent antibody test for rabies.
5c) Mouse inoculation.
5d) Rabies PCR.
5e) Rabies antibody testing.
5f) Negri bodies.
6) How is this disease treated? This section contains the following topics:
6a) What to do with a clinically rabid animal.
6b)What to do if an unvaccinated pet is bitten by a suspect rabid animal.
6c) What rabies treatment is available if a vaccinated pet is bitten by a suspect rabid animal.
7) What is the prognosis for this virus?
8) Prevention of the disease. This section contains the following subsections:
8a) Animal vaccination protocols and schedules (includes some rabies vaccine reaction and side effects info).
8b)Human vaccination protocols (includes information on which people and occupations need the rabies vaccine)
8c) Reducing your exposure to rabies (includes info on what you and your local authorities can do
to reduce the risk of people and pets encountering rabid animals).
9) Rabies in humans. This section contains information on what vaccinated and
unvaccinated people need to do if they are bitten or scratched by a suspect rabid animal. It contains info about post-exposure prophylaxis in people and when it may be required.
10) Considerations when importing and exporting animals from and to affected zones.
11) Rabies-virus links.
WARNING - IN THE INTERESTS OF PROVIDING YOU WITH COMPLETE AND DETAILED INFORMATION, THIS SITE DOES CONTAIN MEDICAL AND SURGICAL IMAGES THAT MAY DISTURB SOME READERS.

1. What is Rabies?
Rabies is a severe, fatal disease affecting the nervous system and salivary glands of dogs, cats, humans, livestock and a wide range of wild mammal species (foxes, wolves, raccoons, skunks and certain species of monkey, bat, civet and mongoose tend to be the sylvatic (wild)
species most frequently implicated in the carriage and spread of rabies). The disease, which has no cure, is caused by a virus of the family Rhabdoviridae, a family which includes several genera one of which, the genera Lyssavirus, contains rabies and also Australian
Bat Lyssavirus (ABLV).
Animals affected by the disease usually die from a range of severe neurological signs. Some will froth at the mouth and drool and make a choking sound, because of an inability to swallow; some animals will become atypically docile; others will become crazy and restless and race around in a mad, disoriented way biting objects and other animals and the air (the classical rabid animal sign - termed furious rabies); some animals will seizure and die and others will progress to a depressed, paralysed
state: unable to move or get up or feed (the paralytic form of rabies), before drifting into a coma and dying. Wild animals affected with the virus may initially appear
'very tame' or be active outside of their normal waking hours (e.g. nocturnal animals may appear in daylight hours), before progressing to the furious and/or paralytic forms of disease.
The neurological symptoms of rabies and the way in which they progress to become fatal
are discussed in detail in section 4b.
Spread by the bite or scratch of infected wild and domestic animals, rabies is a highly contagious disease and one of the animal diseases of major zoonotic risk to the human public. Rabies is found in many countries of the world, including the United States of America, India, much of Europe and also the tropical zones of Africa, South America and Asia. In some of these regions, vaccine and animal
control programs have been initiated to protect the humans and domestic animals living there. The disease is high on the list of severe notifiable diseases in countries (e.g. Australia, Great Britain, Japan and many island nations) that don't yet have it.
2. Which animals are at risk of rabies?
Most non-vaccinated warm-blooded animals of any age group have the potential to contract and die from rabies, however, only certain mammalian species have been found to actually replicate the virus inside them in a way that allows for the spread of rabies from animal to animal (note, the ability of different mammalian species to pass rabies on to other species is variable and is discussed in section 3 - the transmission of rabies).
Domestic mammalian animals:
All domestic mammalian species have the ability to contract rabies. The dog and cat
are obvious and well-known (remember the movies Cujo and Old Yeller, anyone?),
but pet ferrets, rabbits and pet rodents can be affected too. Domesticated livestock
animals (pigs, cows, sheep, horses, camelids) can also contract and pass on the disease to other animals and humans.
Wild mammalian animals:
Because most domesticated animals in rabies endemic developed countries are vaccinated
and thus somewhat protected from contracting or spreading rabies, the main source of rabies infection for humans and their pets and livestock comes from the rabies-infected wild animals that exist in the local area. Unvaccinated domestic animals and humans that get bitten by rabid wild animals can contract the fatal disease.
As with the domesticated animals, any mammalian wild animal species can
be potentially affected by rabies. Wild carnivores (all members of the dog, fox, weasel, cat, civet, skunk, mongoose, raccoon and bat family) are the wild animal species most
commonly implicated in rabies infection and rabies transmission to man, but other wild mammals can also contract and die from the disease. Wild and feral ruminants (cattle, sheep, goats etc.) and pseudoruminants (camels, alpacas, llamas etc.) can contract rabies, as can mammals like monkeys, rabbits, hares and a wide range of rodents (beavers, cavies, squirrels). As is discussed in section
3, the ability of these various species to pass this disease on to other animals and man may vary.
The wild animals which are most likely to be infected with rabies, and which are of most risk to humans and their pets, varies from region to region and country to country and is directly dependant on factors such as:
a) the strain of the rabies virus (certain strains of rabies 'favour' certain wild hosts);
b) the populations of wild animals around;
c) the wild animals' virus susceptibility;
d) the amount of virus shed in their saliva and
e) the location and distribution their natural territories relative to man's.
For example, in regions of the USA that are more human-populated and built-up
(e.g. suburban zones, population-dense townships, outer city regions) rabies infection
is more likely to come from wild animals that have adapted to close-living with
humans (raccoons, skunks, bats and red and grey foxes). In the cold Alaskan wilderness, you are unlikely
to find significant populations of red foxes and raccoons and so the main source of infection is likely to be Arctic foxes and wolves. In other countries, native wolf and fox populations may have been so decimated by environmental destruction and hunting that another species
has stepped into the gap to become the prominent rabies carrier. Some of the countries in Africa and South
America don't have the types of wild rabies-carrier species typically seen in Europe and the USA
and so an entirely different species, common to the area, has taken up the role of
major rabies reservoir (e.g. monkeys, bats, mongooses, civets, cattle).
Non-mammalian species and rabies:
Rabies has been experimentally found to infect and kill a number of non-mammalian
warm-blooded species, including birds. Although the virus will infect these species, only mammalian
species are capable of spreading the virus to other animals and humans. Birds and cold-blooded animals
like reptiles and insects should, therefore, not be a rabies risk to people.
Note - To be safe, I still wouldn't touch a reptile or bird in a rabies endemic area that seemed excessively tame or was acting bizarrely, showing neurological signs or which seemed unwell. The animal might be carrying another
disease of risk to humans.
Humans:
The main reason rabies is such a scary disease is that it does affect and kill
humans. In some parts of the world, where rabies vaccination is unavailable or the
population is too poor to afford it, rabies virus kills thousands of people every
year. Humans can also show signs of furious rabies and there is a theoretical possibility that affected humans could bite other non-vaccinated humans, thereby spreading the disease.
Australian Bat Lyssavirus:
First seen in 1996, this is the only form of rabies seen in Australia to date (though we are always on the
look-out for the first case of 'true rabies' to come into our country). The disease
is a Lyssavirus, closely related to rabies, that is carried by various species
of Australian bats, including four species of 'flying foxes' (fruit bats) and two species of microchiroptera (tiny insect-eating bats). Prevalence of the virus is higher in sick and weakened bats than it is in the general, healthy bat population (carers be cautious)
and bats of any age can be infected. Although the virus does over-time kill many carrier bats, our main concern with this disease is the effect that it
has on people. Unvaccinated humans and, potentially, domestic animals
can be infected by the virus and killed if bitten or scratched (their claws can be coated in infectious saliva)
by affected bats. Thankfully, however, transmission of this rabies disease from non-bat species (dogs, cat etc.) to other species has not been recognized to occur and, thus, the disease
has not become a widespread or high-risk epidemic in this country. Only unvaccinated people who handle bats are at risk of the disease in Australia.
3. Rabies transmission - How is rabies spread and how do animals and humans contract rabies?
During the final stages of rabies infection (around the time that the animal actually starts showing symptoms of rabies) the virus invades the brain and the salivary glands of the infected animal. Consequently, it is the nervous tissue (brain etc.) and salivary secretions of the infected animal that are of infectious disease risk to other animals and humans.
The saliva becomes filled with infectious virus particles which can
be passed on to another animal through the following routes:
1) biting - the infected animal bites another creature and the virus-filled saliva
gets pushed into the open wounds made.
2) infection of an open wound - rabies filled saliva that contaminates a pre-existing
open wound or scratch can lead to infection.
3) infection of the mouth, nose or eyes - the lining of the mouth, nose and eyes of an
animal or human are termed mucous membranes (see images below). The cells lining these regions are not as
tough and impenetrable as normal skin cells and certain strains of rabies virus that make contact with these
regions can pass into the body without the need for an open wound.
4) scratches - some animals (e.g. cats and bats) lick their claws as part of their grooming procedures. Infectious viral particles can pass from the saliva-coated claws into a human or animal should they be scratched by that rabid animal.
5) aerosolized saliva - it is uncommon to be exposed to aerosolized saliva, but in poorly ventilated, enclosed and overcrowded areas (regions with lots of humidity and airborne respiratory
and salivary aerosols), it is possible for humans and other animals to inhale
aerosolised, microscopic saliva particles carrying infectious virions. This can lead to
infection - the virus crosses the mucous membrane linings of the lungs. It is thought that
aerosols are a major route of Lyssavirus and rabies transmission within crowded bat colonies. Aerosolized bat rabies secretions are of risk to people who enjoy hobbies such as caving.
6) ingestion of secretions - occasionally, consumption of infected secretions can
lead to rabies transmission. See point 3 above - mucous membrane spread.
The brain too is full of infectious virus particles in a rabies infected animal. Obviously, it is rare to ever be exposed to these brain-located viruses because the brain is enclosed in the skull, however, infection (by similar open-wound and mucous-membrane contamination routes as saliva) is theoretically possible in humans
that need to dissect the brains of sick animals at post mortem (for rabies diagnosis)
and in humans or other animals that are foolish enough to eat the raw brains
of freshly-killed, infected animals (humans probably wouldn't do this, but wild and domestic animals
might).
Human to human contact and infection has occasionally occurred through strange routes, such as
organ donation, in particular corneal transplantation.


Images of mucous membranes in a dog. The first image shows the pink gums and tongue and
the second image shows the conjunctival membranes (these include the pink tissue under the eyelids
and the thin membrane overlying the 'white' sclera of the eye).
An important note on 'choking animals' and rabies:
One of the earlier signs of rabies infection in some animals (it could even be the first sign witnessed), is the inability of the animal to swallow properly (the throat gets paralyzed by the viruses'
effect on the nerves that control the throat). This inability to swallow results in
the symptoms of drooling and an inability to drink or eat that are witnessed in many rabid animals. Sometimes, the affected animal will have so much trouble that it will start making a gagging, choking noise and action. Many owners and vets mistake this sign as the animal having
a bone stuck in its throat and they will reach into the mouth to grab it
out. Don't do this! This is an excellent way of getting bitten and/or infected by a rabid pet.
How long are rabies-infected secretions contagious for?:
Rabies is actually quite a short-lived virus in the environment.
It is a fragile enveloped virus (this term will be discussed in the next section - how rabies
virus works) and this enveloped structure means that the organism is very susceptible to heat, sunlight, desiccation
(drying out) and most soaps and disinfectants. According to the CDC (Center of Disease Control USA), once saliva secretions are dry the virus particles within
them should no longer be infective - so it's pretty short-lived.
The virus's susceptibility to routine disinfectants (betadine, chlorhexidine, alcohol etc.)
is an important thing to remember in rabies endemic areas. If you or your pet are ever bitten
by an animal that could be carrying rabies, thorough washing and cleansing of the
wounds immediately with an antiseptic solution (e.g. betadine, chlorhex) or soap can go
some way towards preventing rabies infection (because the very first stage of rabies
is local replication and migration of the virus through the tissues at the bite site). Obviously, medical attention must still be sought following a bite, but washing the wound thoroughly in disinfectant is
a good, immediate, at-home step that you can take.
Are other secretions contagious for rabies?:
The other bodily fluids of affected animals, including the feces, urine and blood, do not carry rabies virus particles and so are not infectious. I would be cautious of
any fluid brought up by regurgitation, vomiting or expectoration (coughed-up fluid), however, because that fluid, though not infectious in itself, does have to pass through the mouth
to get out and could, therefore be mixed with infectious saliva secretions.
What about rabies survival in tissues?:
Rabies can remain alive and infectious for several days inside the brain and
salivary glands of a deceased animal, longer if the carcass is chilled in a fridge. This is of importance with regard to infection of domestic and wild animals that might elect to eat a fresh carcass. Freezing and thawing tissues repeatedly will kill the virus.
Can animals be infectious and not show disease signs?:
Yes. It is possible for animals to be secreting the virus in their saliva for up to 5 days prior to the onset of abnormal neurological signs. Consequently, unprovoked bites from wild and domesticated
animals and livestock in rabies endemic zones should always be considered suspicious. Domestic/pet animals should be isolated for a minimum of 10 days, following a biting incident, and monitored for the development of neurological disease signs (most will show the neurological signs within this time). Wild and stray/feral animals should be captured safely and euthanased and their brain tissues sent for rabies testing.
In the case of bats, they can have rabies in their saliva for many months before
the neurological signs develop - bats in all countries (even non-rabies countries like Australia)
should always be considered a rabies risk, even when non-clinical, and bats that bite humans should be euthanased and submitted for testing. It is quicker and easier to test for rabies in the tissue samples of an infected animal than it
is to test for rabies in a not-yet-clinical human or pet.
High risk animal rabies reservoirs:
Some animal species pose a high risk of passing on rabies virus to other animals and humans. This
is probably because these species survive the brain-infection long enough that they are
able to replicate lots of infectious virus particles in their saliva. Domestic (or feral/stray) species of animals that are of higher risk include: dogs and other canids, cats, ferrets and most livestock
animals (in some areas of the world, cattle are a major reservoir of rabies infection).
In the USA, the domestic cat is actually the major domesticated animal reservoir of human infection (more than
the dog) because cats are often permitted to roam and hunt wildlife and their vaccination status is often questionable, compared to dogs. In many third world countries, where routine pet vaccination programs are unaffordable, the domestic dog is actually the major source of infection for humans and other animals: far more than
any wild species is.
In developed countries such as the USA and Europe, domestic dogs, cats and ferrets are
generally vaccinated against rabies (it is the law). Therefore, whilst there is a risk of being infected by bites from unvaccinated domestic animals, it is the unvaccinated feral animals
(esp. stray dogs and cats) and wild animals living near to man that pose the greatest risk of human or pet infection. Wild animal species most commonly implicated in the transmission of
rabies to humans in the USA (and some other countries) include the raccoon, skunk, bat, fox, coyote and wolf. In the USA, the incidence of human infection and/or bites by rabid wild animals probably occurs in that order, with raccoons, skunks and bats being by far the major culprits.
This incidence can probably be attributed to the fact that these species are susceptible to the
virus; shed lots of virus in their saliva; are quite populous in the USA and have adapted to a life around people
(raccoons like to share human food and like to nest in roofs, barns and garbage
areas created as a result of human activities). In contrast, other rabies species less-commonly implicated
in the infection of man, such as the coyote and wolf, are far less populous due to prior hunting, baiting and environmental
destruction activities and are much warier of man and less inclined to live close by.
In places like Africa, Asia and parts of Europe and South America, where skunks and raccoons are not found, the dominant wild animal reservoir of rabies infection is more likely to be a bat
(e.g. vampire bats in South America) or a local canid (e.g. fox, wolf, raccoon dog, jackal or other wild dog species), though monkeys (e.g. marmosets), civets, genets, mongooses and other species can be implicated, depending on the country.
Low risk animal rabies reservoirs:
As mentioned previously, non-mammalian warm-blooded species are rarely affected by rabies and pose a very low risk of passing rabies on to other animals even if affected. Humans themselves are also considered low risk when it comes to passing on the virus:
transmission through biting is remote and very rare and organ transplantation (corneal
transplants) is the main documented route of human to human infection. As far as wild
and domesticated mammal species goes, rodents (rats, gerbils, mice, squirrels, cavies / guinea pigs)
and lagomorphs (rabbits, hares) are considered to pose an exceptionally low risk of transmitting
the disease to man or other animals. It is thought that these creatures die from rabies brain disease extremely quickly - too fast for replication of infectious virus particles to appear in the
saliva. IMPORTANT NOTE - very large rodents such as woodchucks and beavers in the USA have been
found to display clinical symptoms of rabies infection and so should be considered a potential risk to humans.
High risk situations for rabies exposure:
Obviously, some environments and job situations are more risky than others when it comes to
the potential for rabies exposure. The risk of infection is increased in:
a) countries that have rabies - obviously, you won't get rabies in a non-rabies-endemic country (note that bats
are the one exception to this rule because they move from country to country).
b) regions that have high numbers of wild animal rabies reservoirs living in close proximity to people and their pets (e.g. the East coast of America sees the most rabies cases because of a large raccoon and skunk population).
c) countries with minimal or ineffective vaccination programs - in some third world countries vaccination of people and pets is not possible due to unavailability or unaffordability of rabies vaccines. These countries have a high incidence of rabies infection, not
so much from wild animals (though it does occur), but from stray or owned domestic animals (dogs and cats) that wander the streets. Because they are domesticated animals, the number of potential reservoirs in these countries is far greater (tame or semi tame dogs are likely to be very
abundant in a society compared to numbers of wild animal species) than the relatively smaller populations of wild animal reservoirs present in first world countries such as the USA.
d) certain occupations - people involved in animal health industries, rabies research, pest animal eradication and public health work in rabies endemic countries
are at higher risk of contracting rabies. People involved in wildlife rehabilitation - e.g people who routinely
handle bats of all kinds and other wild animals - are also risk. Soldiers and emergency
aid-workers stationed in rabies-endemic third world countries and disaster zones are also at risk from exposure to high numbers of stray and abandoned animals.
e) certain hobbies and job locations - people involved in occupational and pleasure activities
which take them into the habitat of rabies reservoirs are also at risk (hikers, cavers, forestry personnel, woodcutters, campers, people participating in school and summer camps).
A final word of caution for those of you visiting rabies endemic countries (especially
third world countries in Asia, Africa and South America):
If you are planning on sight-seeing and trekking through any country that has rabies, it is always best to contact the disease information and surveillance bureau for that
country before you go. Most travel agencies and local government travel advisory services
can tell you how to contact them. These government disease bureaus can provide you
with vital information about rabies and rabies control in their country including: which species commonly carry rabies; what medical aid is available; where you can go for medical assistance etc.
One important thing to remember about rabies vaccination is that it does not negate
the need for medical assistance, should you be bitten by a rabid animal. Because rabies vaccines are not considered to be 100% effective, even vaccinated people need follow-up rabies therapy if bitten. When going into third world rabies countries, you need to consider the risks of rabies exposure because essential follow-up rabies therapy required, should there be a bite, may not be available in the middle of nowhere.
My advice is not to touch any wild or domesticated mammal in a third world rabies
endemic country, even if you are fully vaccinated against rabies. Not even
seemingly friendly, domesticated pets and livestock. Many countries do not have the high degree of dog and cat vaccination programs that the USA and Europe do and, thus, domestic cats and dogs can be high risk rabies carriers in these
places. Remember that animals can be infectious to man and not yet be showing neurological signs. In particular, I would strongly advise against touching any wild or livestock animals that seem to be excessively and inappropriately 'tame'
or any animal that is acting bizarrely or showing neurological signs (drooling, trouble walking, lameness, falling etc.) or which seems unwell. Some nocturnal
animals with rabies (e.g. skunks) will become active in daylight hours as a result of the virus:
this too must be considered suspicious.
4. What does the rabies virus do to the animal or human? - an overview of rabies symptoms and signs.
As mentioned in the opening sentences, rabies is a viral disease that causes severe, fatal neurological disease in mammals infected with the virus. The following
discussion is mostly for those of you who are interested in how the virus works:
how it replicates; how it infects the nervous system in order to cause the neurological symptoms seen and how it infects and replicates within the salivary glands in order to be transmitted
to other animals. Understanding how the virus works is useful because it
aids your understanding of why symptoms occur; how the disease is spread; what
treatments are available and why the mortality is so high.
4a. How a rabies virus (rhabdovirus) infects and damages a cell:
A rabies virus is a tiny organism (much smaller than a bacteria) which is made up
of a protein shell or capsule (called a capsid) entwined around and protecting a strand of RNA (not DNA). This whole complex (the RNA sequence plus its protective capsid) plus additional free-floating proteins and enzymes (including an enzyme called RNA-dependent RNA polymerase - see discussion below) is contained within a membrane coating (termed an envelope) made up of proteins, carbohydrates and lipids (fats).
What is RNA?
You have probably heard of DNA (Deoxyribonucleic Acid). All human cells have DNA. DNA is a sequence of four different kinds of molecules (A,T,C,G), which can be arranged in millions of different combinations of varying lengths
to code for all of the genes of your body. The information contained in each gene
sequence can be used by the cell as a template or set of instructions by which that cell is able to manufacture certain important proteins and molecules vital to cellular function,
replication and survival. Every cell in the body has the same DNA (every cell therefore contains every gene in the body), but not every gene contained in the
full DNA sequence is switched on (activated) in every cell. Only certain cells use certain genes to guide them in making the proteins necessary for their structure and function.
For example: insulin is a protein coded for by a gene sequence contained in the DNA. The insulin
gene is only switched on in pancreatic cells and the cells of the pancreas use the information
contained in the sequence to enable them to make insulin for the body.
The RNA (RiboNucleic Acid) sequence contained within the rabies virus plays a similar role in the functioning of the virus organism to the role that DNA plays in our own cells.
Similar to DNA, RNA is basically just a strand of protein molecules arranged in various combinations (genes) that code for certain proteins and molecules vital to
virus function, replication and survival. The viral RNA contains sequences (genes) that
code for enzymes (e.g. the RNA-dependent RNA polymerase enzyme) needed in the replication of more strands of viral RNA; internal viral proteins (such as the virus capsid) and various other virus components, including the surface proteins of the virus (the same ones we called antigens in our How Vaccines Work page) which allow the virus to access animal cells.
Unlike bacteria and other, more advanced organisms, viruses do not contain all of the components needed to replicate by themselves. They require a host cell (e.g. a dog cell)
which contains all of the right components required for viral replication. For the sake
of this discussion, animal cells can be thought of as being comprised of three main
regions of viral importance:
1) The cell membrane - the coating (wall) of the cell which acts as a barrier to stop the nucleus and cytoplasm from leaking out and which plays a role in virus attachment and facilitation of virus infection (i.e. viruses must attach to the cell membrane first
in order to access a cell).
2) The nucleus - a region within the cell that is contained within its own thin membrane. It
contains the DNA that codes for all of the functions of the animal cell (see above DNA discussion).
3) The cytoplasm - the 'innards' of the cell that lie outside of the nucleus, but within the main cell membrane. The cytoplasm contains all of the 'equipment' needed to manufacture
proteins and molecules vital to cell function: it is the factory of the cell.

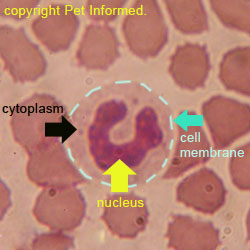
The images show a normal dog white blood cell: the important anatomy of the cell is indicated (cell membrane, nucleus and cytoplasm).
When the rabies virus enters the body of an animal, it attaches to the cell membrane of a particular body-cell-type that it
has been specially 'designed' to invade (i.e. the virus has surface proteins called attachment proteins that allow it
to recognize, bind to and access certain cell types). For example, in rabies, the cells that the virus prefers to invade are the cells of the neurological system and salivary glands
(though it can replicate in non-nervous tissue at the bite site prior to gaining entry into the nerves). When the rabies virus enters the body (generally through a bite), it attaches to a cell
(usually a nerve cell or a local, bite-site tissue cell) that it 'knows' it will be able to replicate within. How does it know? The virus 'knows' because it has special surface proteins contained on its outermost envelope that are specifically designed to only bind to surface proteins that are present on the right kinds of body cells that the virus needs.
It is like having the right key to a door. Body cells with the wrong surface proteins
are not invaded by the virus and are thus unharmed.
When the virus attaches to the right kind of cell, one of two things may happen:
1) the virus outer membrane fuses with the cell's membrane, resulting in the virus capsid and RNA being
released into the cytoplasm of the cell OR
2) the cell membrane reaches outwards, surrounding the rabies virus and its envelope in a 'bubble' of cell membrane (the process is termed endocytosis). This bubble gets released into the cell's cytoplasm where the virus envelope fuses with it, resulting in the release of the viral RNA and capsid into the cytoplasm.
Either way, the rabies virus RNA ends up within the cytoplasm of the host cell.
This viral RNA remains in the cytoplasm of the cell (the region of the cell that contains all of 'factories'
needed to create cellular proteins and molecules). Using one of its own viral proteins: an enzyme
which is not normally present within canine cells (an enzyme called RNA-dependent RNA polymerase), the rabies virus
RNA starts replicating hundreds of identical copies of its own RNA within the animal cell. This process of
rabies RNA replication is a complicated process that involves several steps which, for the purposes
of keeping it simple, we will not go into here (the RNA found in rabies is a special form of RNA termed
negative-sense RNA - it needs additional steps to be able to replicate). The virus also uses the 'cell's machinery' (various cell enzymes and cellular
organelles contained within the cytoplasm) to get the cell to create hundreds of new capsids and viral proteins. Some of these proteins (the surface attachment proteins of the virus) get secreted onto
the surface membrane of the animal cell in readiness for the next stage of the process. The new RNA copies get packaged into the newly created capsids, along with other internal viral elements that the cell has produced. These creations (basically complete rabies viruses without their envelopes) attach to the inside of the animal cell membrane and 'bud' out, taking a
surrounding coating of the animal cell membrane with them (occasionally, the animal cell membrane used
to coat the new virus comes from membrane-coated organelles within the cell, not the cell surface, but this is not important for you to know). This animal cell membrane becomes the new
viral envelope and contains all of the viral surface proteins required to attach to and invade other
animal cells. The cell often dies as a result of the destruction of its cell membrane by the many evacuating viruses.
This repeated process of virus invasion and cell destruction is what causes disease in the animal. In the case of rabies, because the virus needs to make use of the cells of the brain
and salivary glands in order to replicate, this is where the cell damage occurs. Consequently, most of the clinical signs seen in rabies relate to these organs. The more severe symptoms of disease are seen when the immune system fails to kill the virus in time (e.g. an unvaccinated animal) and large numbers of cells start dying as a result of this viral replication.
4b. Effects on the nervous system:
When an unvaccinated animal or human is bitten by an animal carrying rabies virus in
its saliva, the virus remains in the region of the bite site for variable periods of time, sometimes even replicating within the non-nerve local tissue cells (connective tissues, muscle cells etc.),
before migrating to the nerve endings in the region and entering them. The time taken to go from the bite site into the nerve endings can be days to months (in cats and dogs the range is usually between 2 weeks and 6 months, in humans the range can be more than a year). No signs of rabies disease will be seen within this period (it is called the rabies incubation period).
The nerve endings that supply the muscles and skin of the limbs and face (allowing the
animal to move its muscles or feel sensations such as heat, pain, cold and pressure)
are like the ends of long fingers. These 'fingers' (termed nerve axons) arise from a nerve cell located all the way
up in the spinal cord (in the case of the limbs and trunk) or brain (in the case of the face).
The rabies virus migrates from the nerve-ending entry point (near the bite site), up the axon and into the
nerve cell itself, where it replicates (according to Greene CE, this migration up an axon goes at speeds of 10-400mm/day). Replication of the rabies virus in the nerve cell results in injury or death of that cell and, as a result, the animal may display signs of nerve injury as an early manifestation of the rabies infection.
This nerve damage can present as paralysis of a limb or a facial region if the nerve ending invaded had the job of supplying electrical messages to the muscles in order to create movement. Animals bitten on the leg may drag the limb that was bitten and animals bitten on the face might lose the ability to blink or to swallow. This is how the condition 'paralytic rabies', otherwise known as 'dumb rabies', first starts (see section below on paralytic rabies).
Alternatively, if the nerve ending affected has the job of supplying sensation to the limb or face, the animal will not show paralysis as a first sign but, instead, show signs of hypersensitivity of the
bite region (even after the bite has healed over) or loss of sensation (numbness) of all or part of a limb.
It can be difficult to appreciate focal losses of nerve sensation in animals, unless a significant
region of a limb or face is numb (the animal will then start to use the limb differently).
Animals with hypersensitivity and sensory 'pain' of the limb will lick the affected region (often the bite site) to the point of self trauma. This is how the condition 'furious rabies' often starts (see section below on furious rabies).
The rabies viruses replicate in the sensory or muscle-supplying nerve cell body and then bud out of that cell, into the spinal cord, as hundreds of new, infectious rabies particles. From there, the rabies viruses will locate new axonal endings in which to invade.
There are hundreds of axonal endings located within the spinal cord. These are all part of the 'messaging system' that is used by the brain when it directs the spinal cord nerve cells
to tell the limbs to move. For example: electrical messages move from nerve cells located in the brain, down an axon to the spinal cord. Chemical messages cross from the end of that 'brain-derived' axon to the nerve cell of the target spinal cord nerve (whose own axon and nerve-ending supplies the muscles that the brain wants to move). The spinal-cord nerve is stimulated by the chemicals and sends
electrical messages down its axon to the muscles, telling them to move as the brain directed. A similar system of axonal cell-to-cell messaging is also used by sensory cells to relay
messages back to the brain (telling the brain about sensations of heat and pain and pressure etc.).
Rabies viruses enter axon endings (nerve endings) located in the spinal cord and then
travel up them to their nerve cell bodies (where the nucleus and cytoplasm is). These nerve cell bodies might be located in the brain or higher up in the spinal cord
(towards the animal's head). In the nerve cell, the process of virus replication and
cell damage is repeated. More viruses erupt and invade more axons and the process continues.
Eventually, through this process of replication and axonal entry and migration, the rabies
viruses reach the brain. The brain contains hundreds of closely-associated brain cells and millions
of very short axons, in which to gain entry to those cells. Consequently, once the rabies
virus enters the brain, the process of virus invasion and replication really takes off in a big way. It is here, with millions of brain cells being invaded and destroyed, that the symptoms of full-blown rabies really become apparent.
There are a huge range of neurological symptoms that can fit with a diagnosis of rabies. Similar to the neurological symptoms described on our canine distemper page, the neurological signs seen in any one rabies patient really depends on the part of the brain being injured at the time. The rabies viruses can invade any region of the
brain and so, theoretically, any neurological combination of signs might be seen. It is not uncommon for weird, atypical rabies signs to occur in individual animals.
When talking about rabies symptoms, however, there are two major neurological presentations
that seem to be more typical with regard to this disease. These are the furious rabies signs and the paralytic rabies signs.
Furious rabies symptoms:
Furious rabies occurs when the virus manages to reach the brain of the animal without
doing too much damage to the motor nerves (nerves supplying the muscles and movement)
in the process. This possibly occurs as a result of the virus accessing the brain via sensory nerve pathways (whose nerve cells bodies are located in a different region of spinal cord to the
motor pathways) or via more direct routes (for example through the respiratory or nasal pathways - e.g. inhaled and accessed through nasal nerves which go direct to the brain).
The animal will initially display 'vague' signs of 'not being right'. These signs,
termed prodromal signs, may last up to 3 days before the more obvious signs arise. The animal (dog or cat) may have a fever or be off its food. To their owner, the pet might seem to be excessively friendly, docile or clingy compared to normal; the animal might appear overly anxious (esp cats) and choose to hide out in isolated regions of the house or yard or it might seem to be unfriendly and excessively aloof or standoffish. Some animals will vocalize and whine. Some will snap at invisible objects. Formerly nice animals might become snappy and irritable. Fitting with the
idea that sensory nerve infection may be the initial site of virus invasion, some
of these animals will aggressively lick and traumatise the original bite site. This
suggests that the sensory nerve supplying the region is injured, creating imaginary
sensations of pain (hypersensitivity) in the once-bitten region.
Following the vague signs, as the brain of the animal becomes more and more invaded, the animal will soon progress into full-blown furious rabies symptoms. The initial vague signs
will increase in magnitude. The animal's irritability, restlessness and anxiety will seem to
increase as will their tendencies towards aggression or, alternatively, avoiding
man (hiding out in quiet, dark places away from people). People attempting to
approach and capture these animals may be savagely attacked and bitten. The animals may appear spaced-out-looking with dilated pupils and trace-like expressions and they may
seem to be compelled to chew things (they will ingest weird objects like stones and wood and can get them stuck in their gastrointestinal tracts). As the disease
progresses, the rabies affected animals will often become hyper-reactive to sight and sound (animals will often react violently to loud noises and will avoid brightly lit areas). Eventually, the animal will 'go crazy.' Affected animals may run around madly (some will die of heat-stress and exhaustion from endless running) and may attack anything that moves (sometimes even inanimate objects such as cages and doors) - killing other pets and/or
spreading the disease around in the process. Eventually, the brain damage that occurs
will be such that the animal is unable to walk well (it will walk in a drunken, uncoordinated fashion) and may start having seizures.
Animals die as a result of seizures, dehydration (they might not drink or eat) or as a result of the virus finally affecting the nerve centers that control the motor (muscle) system. The animal affected in this way will become paralysed (similar to the paralytic form of disease) and die of
an inability to breathe.
It generally takes 1-7 days for animals showing the furious rabies signs to die. This
is the reason (see section 10 - rabies in humans) why domestic pets that bite humans are
confined and observed for 10 days in order to see if the biting animal carried rabies.
By the time a rabid dog starts to show signs of biting and aggression, the rabies
should be already in the brain and progression of the disease should be very obvious within
the 10 day period.
Wildlife will show similar signs to domestic pets. They may become active in the daytime when they are normally active at night; they may be seen walking out in the open instead
of taking their normal anti-predator precautions; they may look spaced out; they may appear to be atypically 'tame' (don't touch them!) and they may aggressively attack humans and other animals
when approached. Bats clinically infected with Lyssavirus tend to be weak, unable to fly
and suffering from hind leg paralysis.
Paralytic rabies signs (dumb rabies):
Paralytic rabies occurs when the virus manages to reach the brain of the animal via the motor nerves (nerves supplying the muscles and movement), damaging them in the process.
If an animal is bitten on a limb, it will normally show signs of paralysis in that limb
first. The animal may initially seem OK in itself (though it could have vague signs such as fever, inappetence, anxiety or depression), but have a flaccidly paralysed limb (a floppy
limb). As the disease progresses, the animal will often become paralysed in the opposite
limb. This occurs because there is very little distance for the virus particles to travel to get to the nerve bodies of the opposing limb and because the two sides of the spinal cord do have axonal links to each other for the virus to travel along. If the bite occurred on a hind leg, the animal will initially become paralysed in both hind legs. If the bite was on a foreleg, the animal will become paralysed in the front legs first. Eventually, the virus particles
will travel throughout spinal cord, via the motor (muscle) nerve pathways, affecting the remaining limbs
in a similar fashion. Dogs bitten on the hind leg will show a progressive, ascending paralysis
as the virus paralyzes the hind legs and then the forelegs. The brainstem eventually becomes
infected, leading to an inability of the animal to swallow, blink or move its face.
The final stage of the disease comes when the nerves that supply the muscles of respiration become affected (muscle activity is required to expand the rib cage and
lower the diaphragm - the process of breathing) and the animal dies of suffocation.
If the animal is bitten on the face, the paralysis signs will typically involve the nerves controlling the muscles of the face first. The animal may be unable to blink its eyes,
leading to eye ulcers. The third eyelids may protrude across the eyes. The animal may be unable to swallow, resulting in a steady flow of unswallowed saliva pouring from the mouth (drooling). This can result in the animal choking on pools
of saliva contained at the back of the mouth - humans may get the false impression that
the animal has a bone stuck in its throat and be bitten trying to retrieve it. The
animal may even inhale enough saliva to choke to death. The animal may seem to be unable to close its mouth,
exacerbating the drooling. Paralysis of the pharynx (upper trachea and vocal cords)
may result in obstruction of the upper airway and/or a change in the animal's voice. Invasion of the brain soon follows, leading to generalised paralysis and respiratory arrest (as seen when a limb is bitten) or the onset of the furious form of disease,
with seizures and diffuse brain damage being the cause of death.
The disease progression is faster with the paralytic form of disease, with early signs
lasting up to four days and full-blown symptoms lasting around 2-4 days.
Note that the two rabies conditions described above are not mutually exclusive. Animals can just show one form or the other, without there being evidence of both forms of rabies signs, however, it is also possible and common for furious rabies to progress to the paralytic form terminally (near to death)
and for paralytic rabies cases to show signs typical of the furious form.
Rabies in dogs:
Dogs with rabies can show either the paralytic (dumb) form of rabies (as described above) or the furious form of rabies (complete with all of the signs of aggression, aloofness, timidity, wariness, behavioural alteration, self-trauma, seizuring and hypersensitivity to light and
sound described in that section) or a combination of both.
Symptoms of rabies in cats:
Similar to dogs, cats with rabies can show either the paralytic (dumb) form of rabies or the furious form of rabies as described above. In general, the furious form of rabies
tends to predominate in cats. The prodromal (initial) stage of rabies in cats is similar to that
described in the furious rabies section. The cat tends to initially display 'vague' signs of 'not being right'. The cat may have a fever or be off its food. The cat might seem to be excessively friendly, docile or clingy compared to normal or it may, alternatively, become anxious (esp cats), wary, unfriendly and irritable. The cat
may resent handling and human contact and choose to hide out in isolated regions of the house or yard. Some cats will display excessive pupil dilation during this period and
adopt a creepy, trace-like, staring appearance. The furious form of the disease is similar to that described in the furious rabies section. Rabid cats can become
extremely aggressive towards moving and unmoving objects and they can display signs of uncontrolled muscle twitching or tremors and incoordination. Some cats appear driven to run: they
can run around so madly and uncontrollably that it is possible for them to die of
exhaustion and heat stress. Damage to the nerves of the throat can result in an inability to swallow (eat or drink) and these cats may drool profusely. Terminally, these rabies cats may develop fatal seizures or they may progress to the paralytic
(dumb) form of the disease. As with dogs, it is possible for cats to develop
and die from the dumb form of cat rabies without ever showing any signs of furious rabies,
however, this is quite rare (cats tend to be more consistent than dogs with regard to showing
the furious form of the disease).
Symptoms of rabies in humans:
People with rabies tend to show similar signs to dogs and cats with the disease.
There is generally an initial prodromal stage, where the patient might show signs
of fever, headache, restlessness and nervousness and experience painful sensations in
the region of the original bite site. As the disease progresses, human rabies symptoms
appear that are similar to rabies disease in the cat and dog. The rabies victim may become restless, excitable, violently aggressive and hypersensitive towards light and sound
stimuli. The patient will become progressively disoriented. Muscle tremors
and incoordination eventually develop and the patient may drool and experience pain or disability upon swallowing (people with rabies become afraid to drink water because of painful throat spasms,
a condition termed hydrophobia). Death occurs as a result of fitting or progression
to the dumb form of the disease.
4c. Effects on the salivary glands:
Clinical disease symptoms relating to the salivary glands are not generally appreciated
by vets or owners, however, the effect of the virus invading the salivary glands must be noted because this is
the predominant way in which the virus is passed on.
Once the virus has gained entry into the brain, it replicates in the nerve cells that supply axons to the salivary glands of the animal. Virus particles travel
down the axon of the nerve cell to the salivary glands, setting up shop in the glandular
cells of the gland. As the virus particles replicate in the animal's salivary glands, infectious virus particles are shed into the saliva, ready to infect another animal
with the next bite.
The important thing to note about this process is that it occurs quite early. As soon as the
virus enters the brain, one of the earliest things it does is invade the salivary gland nerves, resulting in infectivity. In many cases, the animal is already secreting
infectious virus particles into its saliva before the onset of neurological signs. In dogs, the animal can be secreting virus for up to 5 days before the signs of furious
or paralytic rabies appears and, in cats, the animal can be secreting for up to 3 days
before neurological disease signs appear. In bats, it can be much longer. It is for this reason that bites by apparently normal
animals should be taken seriously in rabies endemic areas. It is another reason why
apparently 'normal' domestic animals are isolated for 10-days following a bite (the signs should start in up to 5 days) and why apparently 'normal' wildlife animals (skunks, raccoons, bats) and stray animals are euthanased and sent off for rabies testing, following a bite, regardless of neurological
symptoms.
4d. Rabies vaccine-associated disease:
The live rabies vaccines have been associated with a range of severe clinical disease
states in animals, as a result of the live vaccine infecting the nervous system. The symptoms seen in this vaccine-induced rabies disease can be so similar to the real
disease that it is impossible to tell the difference between the two (aside from a history that tells you that the animal was vaccinated and not bitten). There are several rabies vaccine-induced disease states that may be seen:
Typically seen canine vaccine-associated rabies conditions:
Coonhound paralysis:
The rabies-vaccinated dog may develop flaccid paralysis of the limbs (a floppy dog):
a condition which mimics many other diseases including tick paralysis, botulism, snakebite and organophosphate toxicity in appearance, but which is closest in pathophysiology to the disease Coonhound paralysis. Coonhound paralysis (medically termed polyradiculoneuritis) is an auto-immune attack on the nerves supplying the muscles of the body, such that the animal becomes paralysed and is unable to move. These animals are paralysed, recumbent and may even be unable to breathe on their own (due to paralysis of the muscles of respiration). These rabies-vaccinated animals, if supported well (e.g. nutritional support, possible ventilatory support, intensive care) may get better, but this might
takes months and could be very costly.
Rabies-vaccine-associated encephalomyelitis:
Dogs vaccinated with live rabies vaccines may also get severe rabies vaccine-virus infection of the brain and spinal cord (called encephalomyelitis), which mimics the rabies disease itself. In this condition, the vaccine virus replicates within and
damages the nerve cells of the brain and spinal cord similar to the way in which true rabies does. Any part of the nervous system can be affected and so neurological signs can be very variable, with symptoms similar to the furious and paralytic forms of the rabies disease even appearing in individuals. This condition will progress and there is no cure.
Typically seen feline vaccine-associated rabies conditions:
Flaccid paralysis:
In cats (and also some dogs) what can be encountered, following rabies vaccination, is a progressive flaccid paralysis, similar to the paralytic form of true rabies disease. The paralysis generally starts in the leg in which the vaccine was given (generally the right hind leg). This paralysis progresses to involve the other hind leg (the cat or dog ends up dragging the hind legs) before eventually involving the forelegs as well as the brain (the animal may seems demented). It is rare to see
a furious phase with this disease condition. There is generally no cure for this progression and the cat or dog will either die or need to be euthanased.
Note - in dogs, it is possible for these flaccid paralysis symptoms to be mistaken for Coonhound
Paralysis symptoms. The two vaccine-associated conditions appear very similar, however Coonhound paralysis doesn't affect the cranial nerves (nerves of the head) and does tend to result in the animal having a lot of nerve pain and hypersensitivity towards
being touched. Of the two, only the Coonhound paralysis condition is treatable. Thankfully, irreversible vaccine-associated flaccid paralysis of the kind described in the cat rarely occurs in the dog. In the dog, live vaccine associated flaccid paralysis is more likely to be the Coonhound Paralysis disease.
When do rabies vaccine associated diseases occur?
If they occur, the vaccine-induced forms of rabies disease generally develop around 10-21 days after receiving a live virus rabies vaccine.
Is vaccine-associated rabies a risk to other animals and humans?
The vaccine-induced rabies diseases, though often terminal to the patient, are not a risk to humans or other pets. The vaccine is not virulent and it is not shed in the saliva
and thus it is of minimal infectious disease risk. The danger of vaccine-associated rabies
comes mostly from the fact that it is impossible (just by looking at an animal) to determine if an animal has true rabies (infectious to man) or vaccine rabies. The risk comes when a person thinks his pet has vaccine rabies and it actually has the real thing!
Prevention of vaccine-associated rabies:
The appearance of vaccine-associated rabies used to be a more common occurrence when
live vaccines were used to vaccinate pets. Because of this side effect, many countries
stopped using live rabies vaccines in favour of killed / inactivated vaccines and recombinant vaccines,
which do not have this problem. Killed and recombinant vaccines are generally more expensive to make
and, unfortunately, this cost puts them out of the reach of some rabies-endemic countries.
Because of this, there are still many countries that are forced to continue on with
live rabies vaccine schedules and, thus, the risk of vaccine-associated disease continues for them.
Other side effects?
Live or killed rabies vaccines can also cause a range of side effects common to many different vaccine types, including anaphylactic shock, injection-site lumps and pain, immune
mediated diseases etc. These are all discussed in our comprehensive vaccine side
effects pages. In particular, read about feline vaccination-associated fibrosarcomas
if your cat has had the rabies vaccine (note, it can also occur in dogs). Rabies vaccines and feline leukemia vaccines are the two vaccine types most commonly implicated with this cancerous condition.
5. Rabies testing - Rabies diagnosis and detection.
Rabies in humans and pets can be a very difficult disease to diagnose in the live individual.
Diagnosis is generally presumed on the basis of the animal or human's history (e.g. vaccination records, previous bite by a suspect animal etc.) and clinical signs,
with final, definitive diagnosis made using laboratory testing (points 5B-5E).
Any animal with progressive neurological signs in a rabies-endemic zone should be
considered a potential rabies carrier.
The virus tends to be present in very low numbers in bite sites, saliva samples and other, easily obtainable tissues, making the virus difficult to detect by routine
saliva-sampling and tissue biopsy means. Also, because the virus likes to hide out inside cells (nerve cells), the body's immune system can't get to it easily in order to generate
a protective immune response including antibodies. Consequently, although blood antibody levels can be used to determine if an animal is infected with many other diseases, in the case of rabies, the anti-rabies antibody response is typically small and measuring them is not a useful
way of determining active rabies infection. Unfortunately for our pets and wildlife, the very best and most accurate tests for detecting rabies with high sensitivity all involve sampling the tissues of the brain. In humans, this might be done in a live individual, but in animals, this generally involves the death of the creature in order to obtain the essential sample.
For some great images of the rabies diagnostic procedures described here, including FA testing
and Negri bodies, visit http://www.cdc.gov/rabies/diagnosis.html
5A) Obtaining the samples - information and advice on the capture of rabid animals; handling and storage of deceased animals; euthanasia of rabid animals and what
you can do if you encounter a wild or domesticated animal with suspected rabies.
Why we euthanase pets and wildlife suspected of having rabies:
Animals suspected of having rabies are generally euthanased and their brains submitted for
testing. In the case of wild animals, stray/feral animals and livestock animals that attack other creatures or man
(even if they have no obvious rabies neurological signs yet) or that are found to be acting bizarrely or in ways typical of rabies, this decision to euthanatise and test them for the virus is an easy decision and a routine part of a rabies control programme. Rapid, highly accurate diagnosis of rabies in the deceased biting animal results
in more rapid, accurately-targeted treatment being provided to bitten humans and animals and, hopefully, a better outcome for the victim. It is far quicker to test the rabid animal at post-mortem than it is to wait for a bitten animal or human to become positive on live-animal/human tests (by the time the victim tests positive, it is often too late to treat them). It is for this reason that wild, stray and livestock animals involved in acts of aggression against humans
or pets should be captured (if this can be done safely) and submitted for tissue sampling.
In the case of pet animals that bite people or that are suspected of having rabies because of the neurological signs seen, the decision is far harder. Owners want to be sure
their animal has that disease, and not some other behavioral or neurological disease, before the animal
is put down and submitted for testing.
In the case of asymptomatic pet animals that bite people,
the animal is not immediately euthanased as a wild or stray animal would be: the animal is
instead confined and monitored for 10 days, looking for the appearance
of any neurological symptoms. If they develop, the animal is euthanased and tested.
In the case of pet animals that attack other people or animals and show neurological symptoms, immediate euthanasia and testing is strongly recommended. This can be very difficult for many
owners to accept. The first difficulty owners encounter when making the decision to euthanase a pet for rabies comes from the fact that many of them don't even realise that their pet has been in an altercation with a rabid animal (not all bites are witnessed) and so to their minds, it seems, "my pet can't have rabies: he wasn't bitten". He was bitten, the owner just never saw it. The second difficulty comes from the fact that there are few highly-sensitive, highly accurate tests available for detecting rabies in the live animal (pre mortem). Those tests that are available to diagnose rabies in live human patients are generally illegal to perform on live animals
because they are not 100% accurate. Owners get very frustrated with the fact that their vet can't offer anything to diagnose rabies in their pet whilst it is still alive.
I have mentioned those pre mortem rabies tests that I know of in this section for completeness, but strongly advise against using them in preference to euthanasia and tissue sampling, unless there are exceptional factors in the history as to why the animal should not have rabies. The reason pre mortem testing should not be done on animals? Because the fact that these pre mortem rabies tests are not highly sensitive means that there is a high possibility of getting false negative test results. This means that, should you choose to believe a negative test result, you could well end up with an animal in your household that is infected with the rabies virus, but you don't know about it.
This animal will then pose a risk to your family and your neighborhood. Unfortunately, even beloved pet animals suspected of having clinical rabies disease are best euthanased and tested properly, to be sure. This is to ensure your own personal safety and that of your family.
IMPORTANT NOTE: The legislation varies from country to country and county to county
as to what you can do with regard to pet animals suspected of carrying rabies. Generally, it is illegal to do pre mortem rabies testing on animals (due to the inaccuracy and public health risk involved), however, the law might be different in your area, so it is worth checking out.
Likewise, most places allow owners to keep non-symptomatic biter pets alive and confined for 10 days
to see if they show any rabies symptoms, however, the law might be different in your
region so you must check this out with them. Euthanasia may be compulsory, depending on the situation and locale.
Aside from the human health and animal health risks involved in letting a rabid animal continue to roam free in the public domain, the other reason why we elect to euthanase rabid animals
(domestic or wild) upon suspicion of the disease is for humane reasons. These animals
die horribly from predation, starvation, paralysis (suffocation) and seizures. It is
much kinder to put them down.
Capturing a suspected rabies animal for samples:
If you have a pet, wild, stray or livestock animal in your yard or area that you suspect
is carrying rabies (maybe it is showing neurological signs, maybe it has made an
unprovoked attack on a human or animal), you need to confine it somewhere
so that it can either be monitored closely for 10 days (non-symptomatic pet animals only) or
collected health authorities (so that it can be humanely euthanased and a diagnosis made).
The capture/confining of the animal is particularly crucial if the animal
has bitten someone (having the animal will allow for a quick diagnosis and rapid
implementation of appropriate therapy).
If the animal is already located in an area that can be easily closed off and the animal confined, then you should confine it so that it can not escape before calling the relevant health authorities.
Rabid animals (e.g. rabid pets) can be enclosed in backyards with good quality fences, rooms of houses or sheds, livestock yards (in the case of livestock) and large cages (e.g. cat traps) etc. Once confined, the animal may become aggressive, biting at the cages or doors, or it may seek out a covered, dark region in which to hide. Either way, do not enter the confined area or attempt to touch, approach or soothe the animal. You could be attacked. Calmly call your local authorities and they will assist you. They
will take the animal away where it can be euthanased humanely and tested for rabies.
Expect your local authorities to be extra cautious around the animal, even if it was
once your beloved pet. Don't be surprised if they instruct you to keep well out their
way: they are not being mean, they are keeping you safe! They may be required to use harsh methods of restraint such as pole-catchers (a noose-like lead on the end of a long pole), heavy padded clothes and cages to capture the animal (pet or otherwise) safely. In extreme cases, they may
even have to resort to shooting the animal with a tranquillizer (or bullet) in your own yard or house, prior to taking the animal away. These measures will be distressing for you if you choose to watch, but are required to keep you and themselves safe.
Very small animals (e.g. bats) can be caught safely by throwing a thick blanket or towel over
them and using heavy gloves to pick the animal up inside the blanket. Be very cautious
of sick bats: they have a high incidence of rabies or Lyssavirus.
If the animal is located in an open-area, non-enclosable space, it is best that you do not
chase it, provoke it, go near it or attempt to 'herd' it towards an enclosed area. Rabid animals, even small ones, are exceptionally fast and aggressive. They do not act like normal animals and have no fear inhibition: you could be savagely attacked and bitten trying to capture one in the open. It is always best and safest to get a professional in capture and/or kill the animal because, one, they are qualified to handle such dangerous
animals and, two, they have often been vaccinated against rabies. The job of capturing
the animal may, in some circumstances, require the authorities to shoot the offending animal
with a tranquilliser dart (prior to euthanasia) or a lethal shot.
If you are located in the middle of nowhere or the animal looks as if it is going to
escape the region well before anyone arrives to help (particularly if you need
that animal's samples for diagnosis because a person has been bitten by it), you can, depending on
your local laws, shoot the animal yourself. Obviously, don't shoot anywhere around people
or houses! Don't try to kill the animal by any means that would require you to get near it (clubbing, knifing etc.). One, you could be bitten and, two, most close combat ways of killing an animal are cruel. Shooting is safest and most humane and must be done with a shot to the body (preferably chest) and not the head. Why? Because head shots open the skull, potentially destroying the tissue samples (you need brain for diagnosis) and potentially exposing you to harmful rabies-infectious aerosols.
How do you store a dead animal for rabies samples?
Obviously, if the authorities come over and take custody the animal themselves, they will
take care of all of the storage and handling and tissue sampling duties for you. Whenever possible, you should always call the authorities in to take care of any rabid
living or dead animals. You don't want to be handling these tissues if you can avoid it.
If, however, you find yourself in the possession of a freshly-deceased suspected-rabid animal or pet,
or you have had to kill one yourself, then there are ways to store it so that the samples remain viable for testing.
1) Contact the authorities FIRST. Usually they will come and deal with the animal
immediately so that you won't have to do any of the next steps (steps 2-7) yourself.
If they can't deal with your animal immediately, they can at least instruct you on the best
ways to handle and store the body safely. Steps 2-8 are a general guide only when it comes
to handling dead animals that require lab testing.
2) Wear thick gloves, a face mask, disposable clothing and eye protection, whenever handling any dead animals (you don't yet know what the animal died of nor how it could infect you!)
3) Put the body into a trash bag (e.g. a large black plastic bin bag) if it will fit.
Most domestic and wild animals will fit into a large bin bag. Try not to splash any blood or secretions onto the outside of the bag. Seal the end of the bag with a tie. Put a second bag over
this first bag for extra safety.
4) If you can get the animal over to an open lab or the health department (e.g. daytime hours)
immediately, do it. Again, ring the authorities first to find out the best
way of transporting the creature. They will also provide you with instructions on where to
take the animal. Basically, the sooner the body is out of your hands the better.
5) If you can not get the animal off to a lab immediately or the health authorities can't pick it up immediately, then you will need to store the body somewhere in the meantime, so that the tissue won't continue to decompose (so that you won't lose your samples).
The fridge is the best place to store a body for rabies testing. Obviously, if you have a second fridge - e.g. a bar fridge or a fridge in the shed (you do not want a rabies animal stacked in amongst your own food!) - that would be best. Make sure you disinfect the fridge well afterwards.
Alternatively, you can ring your local vet or veterinary night service. Most of them
are happy to store bodies in their fridge for a small fee and they can arrange to have a lab pick up the samples from them.
6) DO NOT FREEZE THE ANIMAL. This will ruin your samples.
7) Do not attempt to post mortem the animal or remove the brain yourself. The brain contains infective material (rabies virus). Any attempt to open the skull (especially using tools like saws and drills) can lead to aerosolised infective brain material being released into the air (which you can breathe in).
8) If the deceased animal, suspected of having rabies, is large (e.g. a cow or horse),
I would ring the relevant authorities to deal with it. You can chop off the head and store this on its own, but I would advise against members of the public chopping through the
spinal cord (which can potentially be infective, similar to opening the brain - see point 7).
What if the animal died a few days ago? Can I still get a diagnosis?
Samples that have started to decompose are not as good as fresh samples for the detection of rabies, however, it is still possible to get a diagnosis on some samples up to 4 days after the animal has died (longer if PCR is used). This is particularly so if the animal has been lying in a cool place. It is certainly worth submitting. Best to get the relevant authorities in to pick
up a decomposing body.
5B) Tissue samples - fluorescent antibody testing:
The most accurate and sensitive test for the detection of rabies in the deceased animal
(or human) is the fluorescent antibody test (FA test). Because rabies invades the cells of the brain and salivary glands in order to replicate, it is possible to detect and visualize (by means of special stains) the organism in affected brain tissue samples taken from animals that have succumbed to the disease (samples taken at post mortem). Even animals that are not yet showing obvious neurological signs, but which are secreting
virus in their saliva (i.e. are infective) will normally test positive on FA because, by the time the virus is in the saliva, the brain has become involved.
How does FA tissue testing for rabies work?
As mentioned in section 4A, the rabies virus has certain proteins and molecules present
on its surface membrane (envelope) which allow it to attach-to and invade certain cells of the animal body. These surface proteins/molecules are not only present on the surface
membrane of the virus itself, but they are also secreted onto the surface of any
animal cell membrane (e.g. brain cell) that happens to be invaded by the virus. These surface proteins and molecules (termed antigens) of the rabies virus are the regions of the virus
that are targeted by the rabies-specific antibodies made by the animal immune system. For a great explanation of
antibodies: how they are created and what they do, visit our How Vaccination Works page.
This ability of rabies antibodies to bind specifically to rabies virus antigens
is what is taken advantage of when FA testing tissues for the presence of rabies. Tissue sections taken from animals thought to be infected with rabies are exposed to a solution of anti-rabies antibodies, which have been bound to a special fluorescent dye. If rabies antigens are present within or on the surface of the affected brain tissue cells, the antibody/dye complexes will bind to these antigens on the tissues.
Under special lighting, rabies-positive cells which have bound the antibody/dye
complexes will fluoresce (the dye bound to the antibody is the part that fluoresces),
making the affected cells easy for scientists to spot under a microscope.
Can an animal test negative for rabies with this test and still have the disease?
Yes, this can occur, but these incidents, termed false negatives, are very rare.
They generally only occur if the sample was too old or had not been stored properly
prior to testing. Generally, the sample needs to be quite old to not test positive. Even samples up to 4 days old have been found to still test positive with this test, it is that sensitive.
Can this test be used to detect vaccine-associated rabies disease?
A really handy feature of the FA test is that it can be used to differentiate rabies
vaccine-associated disease from the true rabies disease (thus allowing people to know
if they were at risk of infection whilst their pet was sick). The antigens contained
on the surface of the vaccine-virus are different to those of the true virus. Thus, scientists created antibodies (bound with fluorescent dye) specific to the vaccine-virus
antigens to use in this test. When brain tissue containing vaccine-virus particles is immersed in this vaccine-virus-specific antibody-dye solution, the antibody/dye complexes bind to the brain tissue and a positive result is seen, indicating infection
with the vaccine virus. In contrast, true-rabies-virus-specific antibody/dye complexes will
not be able to bind to the vaccine-virus antigens in the tissue and the tissue will come up negative for the true rabies virus.
Can this test be used to detect rabies in the live animal or person?
In a live person, it is possible to run the FA test on brain samples taken by brain
biopsy (biopsy of the brain is technique not uncommon to modern day human medicine). In the animal, it is also possible to do, but not generally advisable or practical
because of the human health risks incurred in taking the samples and the costs involved.
As mentioned in section 4C (salivary gland signs), the rabies virus particles start to track down the nerve axons of the salivary gland nerves and into the salivary glands, at around the time the neurological disease starts. In addition to this, at around the
same time, virus particles also track down the sensory nerve axons and into the nerve endings supplying the skin. It is thus possible for highly-innervated skin samples
to be taken from living animals and humans and submitted for FA testing. In humans, highly innervated areas include the back of the neck, hands and face. In animals, it is the skin around the sensitive whiskers that can be used.
Unlike the situation with the brain samples, testing for rabies in the skin using FA runs a
greater risk of there being false negative results. It takes time for rabies to build up in the
skin to the point of being easily sampled (much longer than for the brain). Because of
this higher risk of false negatives occurring (remember, misdiagnosed animals pose a risk to man),
this method of pre mortem rabies testing has been only registered for use in humans. Animals must have brain samples submitted instead.
Can this test be used to detect Australian Bat Lyssavirus?
FA testing is currently being used to detect ABLV in brain and salivary gland tissues of bats and infected humans.
5C) Mouse Inoculation:
In order to enhance the sensitivity of the FA test and improve the chances of the lab
examiner being able to detect rabies virus particles in tissues, it is possible
to inject suspected rabies-infected brain tissue samples from one animal or human into another species of animal known to replicate rabies to massive, easily-detected levels.
How it works:
Samples of rabies affected brain tissue (from an affected animal or person), are inoculated into
the brain of a healthy, non-rabid mouse. The rabies present in the sample replicates
very rapidly and aggressively in the mouse brain (far more aggressively than it does in cats, dogs and man), because rodents are extremely susceptible to the virus (see
section 3 on low-risk rabies reservoirs). When the mouse is significantly affected, it is euthanased and its brain is submitted for FA testing. Because mouse brains replicate so many rabies particles (far more than a dog or cat brain), more of the antibody-dye complex will bind to the mouse brain tissue, making it far easier for
the lab examiner to detect a positive result (i.e. he will see more cells glowing). This reduces the chance of a false negative result and improves detection considerably.
Note that the mouse inoculation test has recently fallen out of favour in favour of
other, more humane, methods of testing for rabies. It is now possible to grow mouse brain tissue cells in culture (without a mouse) and perform the mouse inoculation
tests on these cell lines.
The main time that the mouse inoculation test (performed on mouse cells in culture) is performed is when the FA test comes up negative, but suspicion of rabies remains really high. This is particularly so when there is a fear that humans might have been exposed to the virus.
The mouse inoculation test will be used in such cases to increase the sensitivity of
the FA testing procedure. Note that PCR is likely to take over this supportive role in future, because of its extremely high sensitivity.
5D) PCR on brain, saliva and cerebrospinal fluid (CSF) samples:
Advancements in viral genetics studies and in the fields of DNA and RNA mapping have enabled scientists to design tests which are capable of detecting tiny amounts of viral RNA or DNA contained in tissue, cell and fluid samples using PCR. PCR
is a very sensitive testing technique and the presence of even tiny amounts of rabies RNA in a tissue sample is highly supportive of infection with this organism.
At present, rabies PCR is available and is the test of choice for detecting rabies in live human patients. Human saliva, brain tissue and CSF can all be tested using the technique. It is possible to detect rabies in the saliva of live animals using this technique, however, euthanasia of the animal and FA testing or PCR testing of brain tissue
is still preferred because of the uncertainty as to the percentages of false negative
results that can be expected from the relatively new test.
PCR is a valuable test because it is able to detect even small amounts of viral RNA
contained within a sample (i.e. it is much more sensitive than FA testing), even a
sample that has been allowed to decompose for days.
Can this test be used to detect Australian Bat Lyssavirus?
PCR testing is currently being used to detect ABLV in CSF, brain and salivary gland tissues of bats and infected humans.
5E) Blood testing - rabies antibody titers:
Antibodies are protective immune proteins made by certain cells of immune system
to attack infecting viruses and other foreign invaders (for details on how antibodies
are made and what they do, see our How Vaccines Work page). Each individual antibody protein
made is very specific and will only target and attack a particular invading organism. For example: antibodies made against the rabies organism will only attack that organism, no others.
Additionally, it must be mentioned that antibodies are only created in response to the presence of the organism that they are specific to (whether this be the real, wild-type infectious disease organism or a closely-related vaccine virus organism). Put basically, if an animal is never exposed to rabies or a rabies vaccine, the levels of protective, rabies-specific antibodies in its blood will be very low. It is only after actual, intra-body exposure to the rabies organism that levels of antibodies increase. This is the purpose of vaccination - exposing the animal to a safe form of rabies so that its immune cells will create protective antibodies.
One would expect, therefore, that the level of rabies antibodies in the animal's blood
could be used in the diagnosis of rabies infection. If the animal or human has never been
vaccinated for rabies before, then, theoretically, their rabies antibody titres should be low. If that same, unvaccinated animal or human becomes sick with rabies then the rabies antibody levels in the blood should go up. High rabies antibody levels should be indicative of active rabies infection and thus diagnostic.
That's theory anyway ....
The trouble with true rabies infection is that it seldom seems to induce a significant
rise in blood rabies antibody levels within the animal. At least, not until very late
in the disease process. During the 2 week to 6 month incubation period, the rabies viruses hide out inside the cells of the animal brain where the immune system can't get to them easily. Because the immune system of the animal is not exposed to the virus very well, it fails to induce a significant, obvious immune system response and minimal antibodies get made. It is only when the clinical signs of rabies start that the antibodies begin to be made, but, even then, they appear late in
the course of disease (the animal is most likely to be dead before diagnostically significant levels of antibodies are made).
Thus, antibodies are not really an effective or reliable way of diagnosing rabies in
animals or humans.
The one time that antibody testing is useful is in the importation of animals to places of
rabies and rabies free status. Animals are tested for rabies antibodies as an easy way
of detecting whether they have received their rabies immunizations prior to shipping. A certain level of anti-rabies antibodies in the blood indicates that the animal has been vaccinated and that its immune system has responded adequately.
5F) Examination of brain tissues for Negri bodies:
When rabies enters the brain, it replicates in the cytoplasm of the brain's nerve cells. The replicating virus particles cluster together in the cytoplasm, forming a visibly-staining
patch of viral material called an inclusion or inclusion body. These inclusion
bodies, termed Negri bodies in the case of rabies infection, can sometimes be seen
in brain tissue samples that are stained with special dyes.
The detection of Negri bodies used to the main way in which rabies was diagnosed in
animals and humans. The trouble with the test is that only certain cells of the brain seem to develop them (the exact right sample must be obtained); the tissue
sample must be extra fresh and well preserved; they only appear
later in clinical disease (you won't detect them in the non-clinical rabid animal) and they don't
occur in all rabies cases (leading to false negatives). Testing for Negri bodies has
been largely superceded by PCR and FA testing these days and is no longer a highly
regarded diagnostic option for rabies detection.
Other testing methods commonly employed in the diagnosis of other diseases, such as
blood panels and cerebrospinal fluid analysis are not helpful in the detection and
diagnosis of rabies because the findings are not specific to this disease.
6. Rabies treatment.
6A) What can you do if your pet has clinical signs of rabies?:
There is no cure for rabies. Because of rabies' high human health risk and extremely high mortality, animals showing clinical signs of rabies are not treated, but are instead put down. Again, as mentioned
in section 5A, handling rabid animals (even pets) is not advised. You can be bitten. Call in the authorities to take care of any suspect-rabid animal, even a pet.
6B) What to do if an unvaccinated pet is bitten by a suspected rabid animal?:
Remember, a rabid animal does not have to look rabid. A rabid animal could be any
domestic or wild animal that looks completely normal (no neurological signs) and
yet comes over and bites your pet, infecting it.
Unvaccinated pets and livestock that are bitten by a known or suspected rabid animal are generally euthanased. The reason for this is the human health implications of the disease. Unvaccinated animals have
a high chance of developing clinical disease, even with post-exposure treatment. Because their incubation period can be variable (up to 6 months) and they are able to shed
virus in their saliva prior to developing overt clinical signs, the owners of such animals
will be unable to predict when the animal's signs might develop and when the infectious human-risk period might start. This puts the owners of such animals at serious risk of disease
and a euthanasia policy is prudent in unvaccinated pets bitten by rabid animals.
As an alternative to euthanasia, it is possible to contain and monitor these unvaccinated, bitten animals for the appearance of any signs. The animal must be confined and watched for 6 months minimum
(remember the 6 months incubation period for domestic pets), then vaccinated against rabies and then confined for another month after this, before being allowed back out
into the public domain. Look at the next section of text on wound washing (thorough lavaging of wounds is essential to try to prevent these unvaccinated pets from
contracting rabies) and post-exposure prophylaxis.
Please note that individual county and country laws may differ
on the matter and that this 6 month wait and see option may not be permissible in your region.
You need to check with your local authorities on the matter.
Obviously, if the wild, stray or domestic animal that did the biting (the suspected rabies carrier) can be safely captured and tested for rabies, then this might help you
in your decision-making. If the biting animal test positive for rabies, then the above
points apply. If the animal is rabies negative, then you probably will
not have to worry. The scare should make you go and immediately vaccinate your pet
though :-).
6C) What to do if your previously vaccinated pet is bitten by a suspected rabid animal:
Remember, a rabid animal does not have to look rabid. A rabid animal could be any
domestic or wild animal that looks completely normal (no neurological signs) and
yet comes over and bites your pet, infecting it.
1) Wash the wounds:
If your pet is bitten, you need to immediately wash its wounds out thoroughly with a substance that kills enveloped viruses. Remember that rabies spends a bit of time in
the bite site tissues before entering a nerve to cause disease. Rabies virus is also very susceptible
to a lot of easily-obtainable antiseptics and chemicals. If you can really work hard at the first bite and thoroughly lavage those tissues with virus killing
chemicals, then you might go some way towards preventing your pet getting rabies. It is
not 100% foolproof, but it is helpful.
Wound washing is an aggressive action in these cases. It is not enough to simply wipe over the surface of a wound! You need to get deep into the wounds with soaps
and disinfectants and wash every section of the deepest wound pockets (every bit that
could have been contaminated by saliva). This involves blasting the wound pockets with
disinfectant solutions under pressure and doing it for long enough that the virus is exposed to the chemical long enough for it to be killed. A neat veterinary trick
for cleaning dirty wounds out is the needle-syringe technique. A needle placed on the end of a large syringe (e.g. 30ml or 30cc syringe) will allow you to blast tissues with a stream of saline or disinfectant solution at enough pressure to dislodge lots of debris and remove the viruses (particularly if the needle tip is placed very close to the
tissue you are washing). The needle is also advantageous because its length will allow you to access the deepest pockets of the wound.
Antiseptics to use in washing rabies wounds: (Greene CE)
Ethanol at 43% or stronger (this really stings though)
Strong povidone-iodine solutions (betadine is the trade name)
20% soap solutions
Benzalkonium chloride at preferably 1-4% concentration will kill rabies, but these high concentrations are very tissue damaging and should not be used in open wounds.
Open wounds are usually lavaged with a solution under 0.1%.
Blasting wounds with saline (0.9% NaCl) for prolonged periods will also remove contaminants,
but you need to do it for a long period and be very thorough. It would be OK to start with saline for the deep, thorough cleaning (to get rid of the obvious debris)
and then finish off with through lavaging using one of the other chemicals (I like
povidone iodine (betadine) - it is a commonly-used veterinary antiseptic).
Problems with at-home wound washing:
The main issue with at-home washing of wounds is not the technique, but the pets themselves. Most owners can not hold a struggling, biting, crying animal down well enough or long enough
to wash its deep wounds out properly and, thus, home cleaning of wounds is seldom effective enough to
reduce rabies risk. Wound cleaning is painful and there is also a chance that you
could be bitten trying to wash the wounds of a pet. My advice, should you really desire to
get those wounds cleaned out properly (and it really is advisable in suspected rabies bites),
is to take your pet to a vet immediately, get the animal put under an
anaesthetic and get the vet to clean the wounds out properly. This will give your
friend the best chance of having the virus in the tissues removed. Even if the wound only
looks like a tiny puncture (a small hole in the skin), get this done: what might
look like a tiny puncture will often have a lot of tissue damage underneath.
2) Post-exposure prophylaxis:
Vaccinated animals (and humans - see section 9) that have been bitten by a suspected rabid animal are treated using post-exposure prophylaxis (a fancy term for preventative treatment given after a bite). No rabies vaccine is considered to be 100% effective and, thus, treatment for rabies after an exposure is always warranted. Post exposure prophylaxis involves the administration of rabies vaccines after the bite.
In domestic animals, post-exposure prophylaxis involves giving a previously-vaccinated bitten animal a single booster rabies vaccine, following the bite, and then confining the animal for
45 days to monitor for signs (Greene CE).
In humans, the post-exposure prophylaxis vaccine regimen is a lot more involved
than that of pets. Vaccinated and unvaccinated humans bitten by suspected rabid animals are generally given a series of rabies shots (up to five, depending on the individual's prior
vaccine status). They may also be given anti-rabies antibodies (rabies immune globulins) too, if they have not
been vaccinated before. Human rabies treatment is discussed in section 9.
Post-exposure prophylaxis has been trialled in unvaccinated cats and dogs following
a bite by a rabid animal. There was some success achieved in preventing those bitten pets from contracting
rabies, however, because the technique was not 100% reliable and, because of the human health implications should there be a failure of treatment, this kind of therapy
in unvaccinated, bitten animals was not recommended for routine use.
7) What is the prognosis for rabies?
The prognosis for any animal or a human that gets clinical rabies (develops the full-blown neurological signs) is very very poor. Recovery is very seldom heard of. Occasionally, humans have been known to recover using extraordinary medicine and
life support techniques, but these cases are few and far between.
In animals with clinical rabies, the prognosis must be considered exceedingly poor to hopeless. In most countries, the excessive veterinary costs associated with trying to save such a critical animal make it impractical for the majority of animals to get anywhere near the kind of treatment required to save them. Even if the treatment
is provided, the prognosis for rabies is so poor that animals will usually die regardless
of the therapy attempted. In many countries trying to eradicate rabies, it may even be illegal to treat the disease in animals, due to the human health risks. As much as you love your pet, it may be the law in your area that vets or other authorities, when faced with a rabies case, must elect to euthanase the affected animal. There may be no choice in the matter.
Animals with vaccine-associated rabies usually deteriorate, despite therapy, and die, regardless of the treatment given. The one exception is the flaccid-paralysis
auto-immune condition Coonhound Paralysis (termed polyradiculoneuritis) which can
occur as a complication of rabies vaccines. This is a vaccine-induced inflammatory attack on the nerves
that control an animal's motion, resulting in it becoming paralysed, recumbent and
unable to breathe on its own. With aggressive therapy (immune-suppressant drugs, ventilatory support, intensive care), these animals may recover, but this could take months. The costs are usually very high and the risk of the animal getting secondary
problems (e.g. pneumonia, secondary infections etc.) is high, making the prognosis guarded (though significantly better than the prognosis for true rabies and the other
rabies-vaccine diseases).
8) Prevention of rabies - How to prevent rabies in pets and humans.
The above discussions about rabies disease, its grave prognosis and its high human health
risks should have made it very clear to you just how important it is that steps are taken to prevent pet animals and humans from getting this disease. Prevention is far better than cure when it comes to rabies! Prevention of rabies virus involves two key steps: immunization and avoiding contact with potentially rabid animals.
8A) Vaccinating pets against rabies.
In many first world, rabies-endemic countries (e.g. the USA, much of Europe) it can be
illegal not to have your pets (esp. cats, dogs and ferrets) vaccinated against rabies
virus. This is as much for public health and rabies eradication reasons as it is for
protection of the individual pet. If you, dear reader, happen to live in a rabies country where rabies vaccination of pets is not the law, but you can access and afford the vaccine, then I would strongly advise you to get this protection for your pet (and yourself - see part 8B). In fact, it is probably more important
for you to vaccinate your pet (and yourself) in country where rabies vaccines are not the law because
there are likely to be more unvaccinated rabies animals around in the local population (they
pose a higher risk of you or your animal catching the disease).
Rabies vaccines are also particularly crucial when it comes to the lives of pet animals
because of the policy, found in many countries, whereby any unvaccinated animal
that is bitten by a rabid or suspected-rabid animal must be euthanased just in case
it has caught the disease! What this means is that your perfectly healthy, unvaccinated dog or cat might be euthanased, following a bite or scratch by a rabid animal, even if it has not
actually caught the disease. Vaccination will save your pet from this automatic euthanasia policy. It will allow your animal to be given the benefit of the doubt and be treated instead of put down.
In most countries, only killed or recombinant rabies vaccines are available for veterinary
usage because of the risks of rabies-vaccine-associated diseases occurring with the
live vaccines (see 4D). Killed vaccines do not cause vaccine-induced rabies, but can sometimes pose risks of anaphylactic reactions and vaccine-site reactions (e.g. lumps) and cancers (usually in cats) due to the high levels of virus and immune-stimulatory additives (adjuvants)
contained within them (see vaccine side effects page for more info). Recombinant vaccines
are vaccines made up of live, non-harmful pox-viruses (canary pox and vaccinia/chicken pox), herpesviruses or adenoviruses that have been implanted with rabies gene sequences, such that, upon invasion of an animal cell, they trigger the cell to manufacture antigenic rabies proteins. These rabies proteins (antigens) get attacked by the animal immune system, resulting in a protective immune response that is effective against a true rabies virus! Cool huh?
Recombinant vaccines most likely have less side effects in the animal than live and killed vaccines
do, but are likely to be more costly due to the technology involved in their manufacture.
In rabies endemic areas, vaccines are usually administered at 3 months of age for dogs, cats and ferrets (this late start is to avoid maternal immunity interfering with the vaccine) and again
in 12 months time and, from then on, yearly or three-yearly (depending on the type of vaccine administered). Animals in high-risk rabies zones can be given a second rabies shot at 4 months of age, following the 3 month vaccine, to minimise the risk of vaccine failure. Animals (especially cats) are given the rabies needle in the right hind leg because of the risk
of vaccine associated sarcomas. Animals traveling to rabies endemic areas are vaccinated prior to traveling and must have adequate anti-rabies antibody levels in their blood before they can be permitted into the rabies country (see next point and section 10).
10-14 days after rabies vacination, animals may have blood taken into order to assess their levels of anti-rabies antibodies. In the case of animals being imported into rabies countries and from rabies to rabies-free countries, measuring rabies antibody levels prior to importation is the law. This is done in order to prove that the vaccine has been given and that it has actually achieved its desired, protective effect. An antibody level of 0.5IU/ml of blood is considered acceptable (Greene CE). Animals failing to achieve this level of antibody protection are considered improperly vaccinated
(they will need an immediate booster shot) and unsafe to import into a rabies endemic zone.
It is important to remember that rabies vaccination in humans and pets is never considered
to be 100% effective. All commercial vaccines need to have an effectivity of around 90% or above
in order to be registered, but no rabies vacine should be considered 100%. Thus, if you or your pet are bitten by a suspected rabid animal, you must
see your doctor or vet respectively, following the bite, to get some post-exposure treatment. See section 6 for animal treatment and section 9 for human treatment.
Note that wildlife and feral or stray dogs and cats can also be vaccinated against rabies.
In many places, vaccinating these animals is a key element to any successful rabies eradication and control program. The vaccines used tend to be oral vaccines, given in
baits.
8B) Vaccinating humans against rabies.
Not all humans in rabies endemic countries are vaccinated against rabies (not even in
first world countries such as the United States). Generally, rabies vaccines are reserved for people at high
risk of being exposed to rabies or Lyssavirus and for people requiring post-exposure prophylaxis (treatment given to people who are exposed to rabies through a bite or scratch by an animal - see section 9).
People advised to get rabies inoculations include: laboratory technicians who study and work with rabies viruses for scientific and commercial purposes; people who work
in diagnostic labs where rabies testing and diagnosis is performed on tissue samples;
veterinarians; veterinary staff; vet students; cavers; wildlife carers and wildlife handlers; animal
control personnel (e.g. rangers, pound operators, shelter personnel); biologists; holiday makers traveling
to rabies zones; soldiers and foreign aid workers traveling to rabies zones and people of any other profession where chances of exposure to a rabid animal is likely to be high.
These at-risk people are given a course of 3 vaccines (days 0, 7 and 14). These rabies shots are
given intramuscularly for best effect, but can be given intradermally as a lower-cost
alternative for third world countries.
Depending on the frequency of rabies exposure expected (this depends on the type of profession - scientists that study rabies and vets in rabies endemic zones have a high risk of exposure, whereas people who visit a rabies country once or twice have a low risk), vaccinated people may have to be blood tested regularly, anywhere from 6 monthly to 2 yearly,
to determine if they are maintaining adequate antibody levels in their blood against
rabies. If their levels of antibodies are found to be insufficient, a booster vaccine is
given. Boosters are generally needed more frequently with intradermal vaccines.
8C) Reducing exposure of people and pets to rabies.
Reducing your and your pet's exposure to rabies can be achieved in many different ways, some of which are under your direct control and some of which are under the control of the public health
services in your area.
1) Things you can do to reduce your pet's exposure to rabies:
A) Be careful where you walk your pet.
Walking animals in high-risk rabies zones (e.g. forested places with high skunk, raccoon and fox populations)
can increase the risk of your pet coming across a rabid animal. If you do walk your
pet in these locations, keep your animal on a lead. This way, if you do encounter
a wild animal on your walk (which could be rabid), your pet will not have the opportunity to chase or provoke that animal.
B) Don't attract wildlife or stray/feral animals to your doorstep.
Leaving bins and foodstuffs outside your house in easy-to-access places will soon attract animals such as dogs, raccoons and skunks close to your home to
scrounge for food: these animals are all potential rabies carriers. Similarly, putting food and milk out for stray cats and dogs might also invite this unwanted virus to your door. Pet food dishes containing uneaten dog or cat food
left outside, as well as dog bones left in the backyard, can also attract unwanted
visitors.
The habitat around your home is also a factor in attracting animals to your house. Dense, heavily-treed gardens provide good cover and housing for unwanted critters, including skunks, raccoons and foxes. Keeping your garden neat and the foliage not-too-dense
may help to reduce this risk of unwanted wild creatures moving in. Barns, gaps under the house and piles of
junk (e.g. old car bodies, machinery) can often be taken up by such animals as they
seek a place to hide or nest in. Again, keeping your yard, barn and shed uncluttered and
preventing animals from getting under your house can reduce the risk of these creatures setting
up a home close to your pets. The type of trees in your yard and local region can also
be a factor in attracting animal pests. In Australia, for example, the kinds of bats
most commonly implicated in carrying Australian Bat Lyssavirus are fruit-eaters. They
are attracted to yards and properties by the presence of fruiting trees. No fruit trees, no bats.
C) Do not allow your pet to eat dead animals.
You will never know why a dead animal found during a walk in the park or forest died. It might have died from predation or sickness or ... it might have died from rabies. It is important, therefore, to never let your pet consume dead wildlife or livestock.
All manner of nasty diseases can be picked up from the consumption of carcasses and
rabies is one of these.
D) Do not contribute to the stray animal population.
Stray and feral dogs and cats are a major rabies risk in human-populated regions, whether it be in first world or third world countries. This is because they exist so
closely to humans and because humans don't usually fear them (people know not to touch
skunks and raccoons, but how often do you see someone reach out to pet an unvaccinated stray puppy or kitten - that animal could have rabies!) You can help to reduce the numbers of stray animals by having your pets desexed and by not dumping unwanted dogs, cats, puppies or kittens into the wild. Take them to a shelter if they are unwanted.
E) Keep your pets inside, particularly at night.
Aside from those rabies-affected wild animals, which start to move about in the daytime as a side effect of their neurological disease state, many of the wild rabies disease carriers tend to be more active in the nighttime. This is when humans are scarce and when their prey becomes more active. During the night, these
animals are more likely to be active around your house and yard, looking for food. Keeping your dogs and cats inside at night can reduce the chance of your pet encountering a rabies-carrying wild animal.
F) Don't let your cat (or dog) hunt wildlife.
In many developed countries, the USA included, the domestic cat has become the main
domestic animal reservoir of rabies infection for humans. Part of the reason for this is
that cats are often permitted to have free-run of the world outdoors: a world which
includes places well outside of the range of your own safe backyard (you try keeping a cat in backyard!).
Roaming cats are apt to encounter wild animals (they may even be actively hunting these animals)
and, as a result of this sort of interaction, many cats become infected with rabies.
2) Things you can do to reduce your own exposure to rabies:
A) Be careful where you go.
You are far more likely to encounter a rabid animal if you are walking in rabies endemic
regions where there are large populations of wild animals or large stray/feral dog
populations. Walking in forests obviously increases your risk, as does going into
villages and slums in third world countries (e.g. India) where there may be large
stray dog populations and poor vaccination programs. Hobbies such as caving, rock
climbing, hiking/bush walking and camping can also increase the risks. Obviously, the threat
of rabies should not be a barrier that prevents you from seeing the world or enjoying your hobbies,
just make sure that you take precautions (get vaccinated, wear protective gear etc.)
and don't take unnecessary risks (e.g. petting wild or roaming creatures).
B) Wear protective clothing in high-risk situations.
People walking through areas where there might be rabid wildlife or rabid stray
animals may reduce their risk of sustaining a serious bite by wearing protective clothing. Thick, full-length trousers and hardy, enclosed footwear (e.g. boots or gum boots etc)
may prevent a bite to the legs from piercing the skin, as might a long-sleeved coat.
When traveling through enclosed spaces (e.g. bat caves) where inhaled, infectious aerosols
might be a risk, wearing appropriate face masks and goggles is advisable, so as to not
let the virus particles access the mucous membranes of the mouth, nose or eyes.
C) If possible, avoid handling wildlife.
Bats and other wildlife can pose a serious risk of rabies or Bat Lyssavirus. It is
highly recommended that you do not approach or try to touch wild animals in rabies
endemic zones. Do not touch bats in any country, even a non-rabies country (most
non-rabies countries have some form of bat Lyssavirus). Remember that wild animals can be infectious, but show no clinical signs (especially bats). Even injured wildlife should not be handled. People involved in the care of wildlife should certainly be vaccinated against rabies before handling any animals
and, even then, handle them with utmost caution and protective clothing (e.g. gloves).
D) Do not approach or attempt to handle stray dogs or cats in rabies endemic areas.
E) Don't attract wildlife or stray/feral animals to your doorstep.
F) Do not contribute to the stray animal population.
G) Owning of wildlife is not advisable.
H) Don't forget to vaccinate the cat!
In many developed countries, the USA included, the domestic cat has become the main
domestic animal reservoir of rabies infection for humans. Part of the reason for this
is that cats are permitted to hunt wild creatures more than dogs or ferrets are. Another part of the
reason is that cats often go under vaccinated and, thus, unprotected in house-holds, compared to dogs.
3) Things your health department can do to reduce rabies exposure to pets and people:
A) Eliminate or reduce feral or stray cat and dog populations:
In many countries, feral / stray cats and dogs are a big problem and a major reservoir
for rabies infection in humans. These animals live in close association with humans
and their pets (they are unafraid as wild animals are), breed rampantly and are
highly likely to attack other dogs and cats that they are unfamiliar with (e.g. your pet!).
Many countries with large numbers of rabies-carrying stray cats and dogs are unable to
afford oral vaccine programmes and must resort to reducing the risk of rabies by reducing the animal
populations themselves. Reducing stray animal numbers can be achieved by combinations of trapping and culling (shooting, baiting etc.) and also by cheap desexing programs aimed at desexing household pets so that more puppies and kittens are not born only to be dumped. Note that animal control programs used alone are
seldom highly effective in eradicating rabies - the best results are achieved when animal control is used in conjunction with oral vaccinations.
B) Eliminate or reduce wildlife populations:
Always a contentious issue, some control may been achieved when highly-populous
wild animal rabies reservoirs are eliminated from habitats close to human settlements. This can be achieved by means of trapping and relocation; culling (shooting, baiting)
and, potentially, chemical desexing programs. Note that animal control programs used alone are seldom highly effective - the best results are achieved when animal control is used in conjunction with oral vaccinations.
C) Oral vaccination programs:
Because some low-virulence (non-disease causing) live rabies strains are capable of crossing the mucous membranes (pink skin of the gums, mouth and intestinal tract), they can be fed orally to an animal in order to vaccinate it against the real disease.
In a similar fashion, recombinant vaccines (live viruses carrying rabies genes) can
also be fed orally to animals in order to vaccinate them. Currently, wealthier countries,
such as the USA, parts of Europe and some other countries vaccinate wild and feral/stray
animal populations by means of vaccine-impregnated food baits. This has gone a big
way towards eradicating rabies from certain regions.
D) Rabies vaccination legislation:
The USA and many other rabies countries have included rabies vaccination as part
of their public health legislation. In many places, it is illegal for domestic dogs, cats
and ferrets not to be vaccinated against rabies. This is to protect their owners and
to protect the wider public. With more animals in the local population being vaccinated,
as a consequence of this law, there is a reduced chance of humans and their pets coming into contact with rabies affected domestic animals.
E) Wildlife legislation:
Many countries have laws about keeping and/or caring for wild animals. Naturally, such laws are designed to protect wild animals from being exploited and kept in unsuitable conditions by people not skilled in their care. However, there is also a secondary
bonus to laws which restrict the ownership and care of wild animals: the protection
of the public. Wild animals carry many diseases, including rabies, which can be of
risk to the inexperienced carer and pet-owner. By making the laws strict on the ownership and care of such animals, authorities can reduce the risk of people being exposed
to these wild animal diseases. In Australia, for example, it is illegal to keep most
wild animals, unless you are a registered wildlife carer with up-to-date training and
a licence to keep animals. People attend courses and training sessions to obtain this experience
and qualification. These carers are educated about the Australian rabies-related disease, Bat Lyssavirus (ABLV), and are vaccinated against it. Non-qualified members of the public are not permitted to keep wild animals: this fact alone protects them somewhat from getting diseases like ABLV, which they have not been vaccinated against.
F) Enforce legislation requiring dogs to be on lead in public:
Animals on leads are less likely to be involved in altercations with other wild and domestic animals and are, therefore, less likely to be bitten by rabid animals.
G) Environmental management and good suburban planning:
Consideration of human and wild animal interactions should be made when councils and city-planners
plan for new urban developments and new recreational areas. As human housing encroaches
more and more upon wild reserves and wild animal habitats, the animals in those areas come under increasing pressure to find food, nesting sites and shelter. As the wild areas dwindle
and these resources become scarce, many animals are forced
to seek out shelter and food in human-inhabited regions. This puts people and
their pets (particularly those people living nearest to the reserves) at ever-increasing
risk of encountering a rabid wild animal. City plans allowing for the preservation of
wild animal reserves and adequate habitat (enough to cover the food, shelter and reproductive needs of the animals living there) will tend to keep these wild animals
in the wild and out of human suburbs. Remember, wild animals don't choose to be around
humans: they avoid us when they can.
9) Rabies in humans:
Although this site has been intended as a veterinary site, with much of the focus
on dogs and cats, no discussion about rabies virus would be complete without making
some mention of the human health implications involved. Rabies is a very nasty disease
that kills thousands of humans every year in developing countries. As discussed
in the previous section (section 8), prevention of rabies is very important because
the mortality for the clinical disease (even in first world, developed nations) is so high. Prevention of rabies in animals and humans involves immunization and reducing
exposure to rabies carriers.
This section (section 9) contains information about you need to do, should you be bitten or scratched
by an animal suspected to carry rabies. Remember, of course, that the rabies carrier could
be any domestic, stray or wild mammal and that it does not need to be displaying any typical rabies symptoms to be infectious to you.
IMPORTANT! Please remember, dear reader, that this site is a veterinary site, intended for educational purposes. The site is not written by human doctors or specialist rabies health professionals. Should you be bitten or scratched by an animal or exposed to a suspect-rabid animal in other ways (e.g. aerosols, caves), in a rabies endemic zone, you should immediately contact a doctor or local health care professional. They will instruct you
on the best thing to do next.
What to do following a bite or scratch by a rabid animal:
1) Wash the wounds thoroughly:
Following a bite or scratch, you must immediately wash your wounds out thoroughly. Remember that rabies viruses spend a bit of time in bite site tissues before entering the local nerves (the first step on the way to causing disease). If you can act quickly (immediately after the bite) and thoroughly wash your wounds out
with a virus killing antiseptic, you may go some way towards preventing yourself
from getting rabies. Wound washing, even if you do it immediately, is not 100% foolproof (you still need to seek medical attention), but it is helpful.
Wound washing is an aggressive action. It is not enough for you to simply wipe over the surface of a wound! You need to get deep into the wounds with soaps
and disinfectants and wash every section of the deepest wound pockets (every bit that
could have been contaminated by saliva). This involves blasting the wound pockets with
disinfectant solutions under pressure and doing it for long enough that the virus is exposed to the chemical long enough for it to be killed. A neat veterinary trick
for cleaning dirty wounds out is the needle-syringe technique. A needle placed on the end of a large syringe (e.g. 20ml or 20cc syringe) will allow you to blast tissues with a stream of saline solution at enough pressure to dislodge lots of debris (particularly if the needle tip is placed very close to the
tissue you are washing). The needle is also advantageous because its length will allow you to access the deepest pockets of the wound.
Antiseptics to use in washing rabies wounds: (Greene CE)
Strong povidone-iodine solutions (betadine is the trade name). Note that some people are allergic to betadine solutions - be cautious using them and discontinue
if irritation and redness of the skin develops.
20% soap solutions
Ethanol at 43% or stronger will kill rabies virus in tissues, but may hurt a lot and be very tissue irritant
Benzalkonium chloride at preferably 1-4% concentration will kill rabies, but these high concentrations are very tissue damaging and should not be used in open wounds.
Open wounds are usually lavaged with a solution around 0.1%.
Blasting wounds with saline (0.9% NaCl) under pressure (see needle-syringe technique)
for prolonged periods will also remove contaminants, but you need to do it for a long period and be very thorough. Saline will not kill the virus, so must be followed up with a chemical disinfectant (antiseptic).
A good technique for cleaning rabies wounds might be to start off with saline for a deep, thorough cleaning (to get rid of the obvious debris and saliva) and then to finish off with a through repeat lavaging using one of the other chemicals (I like
povidone iodine - it is a commonly-used medical antiseptic). The more thorough
and aggressive you can be, the better.
Please remember, this information has been written by a veterinarian, not a human
medical service provider, and is provided for general education purposes only.
As a general principle, all animal bite wounds (aside from snake bite wounds) should be washed as soon as they occur, in order to prevent infection (not just rabies). If you suspect that the biting animal might be a rabies carrier, you should wash your wounds out immediately and thoroughly at home, as described above, (strong betadine solutions, soap solutions and saline under pressure are good choices if you have them), and then immediately seek medical attention. Why? Because it is difficult to wash your own wounds out properly (particularly if they are large wounds): washing them is painful and the wounds can be very deep. By seeing a doctor for repeat wound treatment, you will
improve the chances of removing rabies viruses from your tissues, because the doctor will have better access to rabies-killing disinfectants and s/he will be able to wash your wounds more thoroughly, removing anything that your at-home cleaning might have missed.
Also, your doctor will be able to initiate post-exposure prophylaxis: an important
treatment aimed at preventing you from getting rabies should wound washing fail.
Take home message: If you are bitten by a rabid animal you must wash your wounds out at home as thoroughly as you can and then immediately go to a doctor for repeat wound washing
and post-exposure prophylaxis.
If you are in the middle of nowhere when the bite occurs or you have no immediate access
to a doctor, then thorough at-home washing will help you to reduce your risks while
you seek out a doctor. Obviously the lavaging of your own wounds will have to be very thorough in this situation, because there may not be a doctor available to do
a superior follow-up wash. Take your time and do it properly. In such a situation, I would strongly advise at least ringing a doctor to find out what antiseptic solution
and concentration of solution is best to use.
2) Confine the rabid animal if it is possible and safe to do so:
If the suspect-rabid animal can be safely confined somewhere or safely captured or killed, then
this is advisable. Capturing or confining the biting animal should be done, if possible,
so that its brain can be sent off to a lab for rabies testing. Testing of the biter animal will let you and your doctor
know if you have been exposed to the virus and, thus, tell you what further treatments are required.
The safe capture and/or killing of suspect-affected animals has been discussed in section 5A. The main thing to remember is that these animals can be very dangerous and insanely aggressive. It is not worth getting
yourself or another person hurt trying to capture a rabid animal. If you have any doubt at all about your ability to capture/confine such an animal safely, then I advise
that you do not attempt the capture yourself. Ring your local health authorities for advice and assistance. These people are trained and equipped to deal with dangerous animals.
3) Contact your local rabies public health authorities:
Any incidence of wild or domestic animal aggression should be reported to the relevant animal control and rabies authorities in your region. Obviously, if you are able to confine/capture the animal or the animal is still in your area, you will
have notified the authorities already to come and deal with it. However, even if the
animal was unable to be captured or if it left the scene, the public health authorities should still be notified.
4) See your doctor immediately for post-exposure prophylaxis.
Regardless of whether you have been vaccinated against rabies or not, you still need to see
a doctor immediately, should you get bitten or scratched by a suspect-rabid animal.
This is so that the doctor can treat your wounds (see point 1 in this section) and so that the doctor can administer post-exposure rabies treatment to you.
Post-exposure prophylaxis is treatment given to someone who has been potentially exposed to rabies via a bite or scratch (or another route - see section 3). It is given to unvaccinated people to try to prevent them from contracting the disease. It is also given to rabies-vaccinated people, just in case their previous rabies immunisations
have been ineffective at preventing the disease (no rabies vaccine is
considered to be 100% effective).
Post-exposure prophylaxis in unvaccinated humans:
People who have not had a rabies vaccine previously are given a course of treatments
following a potential rabies exposure.
Firstly, they are given a human rabies immunoglobulin (HRIG) solution
containing antibodies against the rabies virus. This is injected into the tissues around the bite
site (the hope is that the antibodies will mop-up virus particles present in the tissues of the bite site before they can get access to the nerves) and should be administered
as soon as possible within the first week following the bite.
Secondly, these
people are given a series of rabies vaccines (so that they will make their own antibodies
against the virus). These are administered on days 0 (less than 24 hr after the bite is best), 3, 7, 14 and 28. They are given into the deltoid muscle of the arm.
Post-exposure prophylaxis in vaccinated humans:
People who have had a rabies vaccine previously are given a course of vaccines
following a potential rabies exposure, but no human rabies immune globulin (HRIG) solution.
Their series of rabies vaccines are administered on days 0 (less than 24 hr after the bite is best)
and 3. They are given into the deltoid muscle of the arm.
Note: if the animal that did the biting was submitted for testing and is found to be negative on FA testing (see 5B), the post-exposure rabies treatments can stop.
Note: Post-exposure prophylaxis is not innocuous. People can suffer from severe allergic reactions,
fever and painful injection site reactions as a result of the series of vaccines
being given.
What kinds of exposures warrant post-exposure prophylaxis (PEP)?
This is a difficult question to answer because not every aggressive rabid animal shows obvious clinical
signs of being affected with rabies and not every aggressive animal has rabies! Many human doctors choose to err on the side of caution when it comes
to rabies and treat anyone who has been bitten or scratched by an animal with PEP. This
safety precaution is understandable (both from the doctor's and patient's point of view)
but it probably means that a lot of people are given the therapy when they don't need it. As a general guide, the following situations are indications for post-exposure treatment:
1) Any bite or scratch from a stray or feral dog, cat or ferret.
2) Any bite or scratch from a dog, cat or ferret with neurological signs.
3) Any bite or scratch from a wild carnivorous mammal.
4) Any bite, scratch or possible mucous membrane exposure (e.g. aerosols) from a bat. In the case of bat rabies, transmission has been found to occur with no obvious bite, scratch or
mucous membrane contact episode witnessed. Consequently, PEP is advised in any cases of bat exposure where there is the remotest chance of transmission having occurred (even if an 'incident'
of transmission was not witnessed).
These animals should be immediately euthanased and tested following the incident, where
possible.
With bites from owned pets (dogs, cats or ferrets), the need for post-exposure treatment
will vary depending on the history of the animal (vaccine status etc) and the individual situation.
People will often not seek post-exposure treatment if an owned, cared for animal
bites them, however, the wiseness of this really does depend on the individual situation. For example, I would be very concerned about rabies in a pet, if the bite was completely unprovoked.
My advice, in the case of pets, is for people bitten by pet animals to consult with their doctor and/or rabies health authorities first before making any decision not to seek treatment. The animal should be confined for at least 10 days and the development of any neurological signs within that animal should be cause for the animal to be euthanased and tested and for the human bitten to
seek immediate medical attention.
With bites from small rodents (mice, rats, squirrels), there is often little chance of the animal passing on the rabies virus. Thus, post-exposure treatment is often not merited for people bitten by these animals. The best thing to do, following a bite from one of these creatures, is to ring your local doctor and/or public health
authorities for advice.
10) Shipping animals from non-rabies zones to rabies zones and from rabies zones to non-rabies zones:
This can only be a general overview of the procedures involved in the importation and exportation of animals into and out of rabies endemic zones. The reason for this generality is that the rules involved in moving animals between rabies and non-rabies countries
differ from country to country and even between countries. Levels of animal
identification required, vaccination schedules required, post-vaccination antibody testing required
and duration of animal quarantine periods all differ from country to country. If you are
seeking to move any pet or breeding animal from one country to another, it is best that you contact the destination country's embassy and health department for details
on what is involved.
Prior to moving any animal into new country (particularly moving from a rabies to a non-rabies country), there is a lot of paperwork that must be filled in and a number of important criteria
that must be met and procedures that must be performed. Generally, the animal must first be examined and vaccinated by a veterinarian in the country of origin. This veterinarian can not just be any local vet: he or she must be specially accredited (licensed) to perform rabies exportation procedures.
An animal transport form is filled in during this examination. It contains the
following information:
1) Identification of the animal:
The owner's details, the animal's details (name of animal, species, breed, sex, age and markings) and the animal's microchip number are all included on the form. Note that the
microchip given must be of a special brand that is able to be read by all international microchip scanners.
2) Health check:
The veterinarian must check the animal over thoroughly and pronounce it healthy
before it can travel to a new country.
3) Vaccination details:
The animal is vaccinated with a rabies vaccine during the visit and the vaccine details
are written on the form. Details include the date of vaccination, the type of vaccine
administered, the batch number of the vaccine given, the expiration date of the vaccine, the vaccine manufacturer and the rabies vaccination tag number (this is the number contained
on a dog tag that will be fastened to the animal's collar following vaccination, as
an additional way of confirming that it has received the vaccine).
4) Veterinarian's details:
The veterinarian must sign the rabies vaccination form and write down, in the spots provided, his or her details and rabies accreditation number.
With regard to vaccination of the animal, the following rules apply (Greene CE):
1) Puppies must be vaccinated at or after 3 months of age. With certain destination
countries (e.g. Australia), no dogs under 6 months old will be permitted into the country.
2) Kittens must be vaccinated at or after 2 months (if the vaccine is a recombinant vaccine) or at or after 3 months (if the vaccine is a killed vaccine). With certain destination
countries (e.g. Australia), no kittens under 6 months old will be permitted into the country.
3) If the animal is older and has never before been vaccinated, it needs to have 2 vaccines administered 3 months apart.
4) If the animal is older and has been vaccinated before (is up to date), it needs
to have a booster shot 3 months - 12 months prior to traveling.
5) No vaccine should be given within 90 days (3 months) of traveling.
6) 10-14 days after vaccination, the animal is blood tested to determine whether
its immune system has responded to the vaccine and made adequate amounts of anti-rabies antibodies.
Antibody measurements must be performed under strict conditions of laboratory testing;
laboratory quality control and animal labeling and identification (e.g. microchip numbers
are included in lab identification forms). Animals must achieve an antibody level
of 0.5IU/ml in order to be accepted for shipping and no animal can be transported
until 90 days AFTER the lab has received the blood samples.
7) Depending on the destination country, there may be an additional period of time
required, following receival of the antibody test results, before animals will be permitted into
the country. For example, in the case of Australia, 180 days must pass, from
the time of antibody testing, before the animal can be permitted into the country.
Once the animal has entered the new country, it is then placed into quarantine. The period of quarantine time required varies from country to country and depends on factors such as prior vaccination status and the animal's country of origin.
Quarantine can last from 1-6 months, depending on the destination country's rules and the circumstances surrounding the animal.
11) Your rabies links:
For a good paper on Human Rabies Prevention and Treatment:
http://www.cdc.gov/mmwr/preview/mmwrhtml/00056176.htm
For info on rabies statistics in the USA, visit:
http://www.cdc.gov/rabies/epidemiology.html
For some really neat Frequently Asked Rabies Questions:
http://www.cdc.gov/rabies/qanda/general.html
For some nice Q and A about Bats and Rabies:
http://www.cdc.gov/rabies/qanda/bats_camps.html
For more on Rabies Diagnosis (incl some great pics of FA
testing and Negri Bodies):
http://www.cdc.gov/rabies/diagnosis.html
To go from this page to our homepage, click here.
Putting up this page for you has been a great learning experience for me too. As a veterinarian in the great, sunny land down under (Australia), we don't actually see rabies.
We do get the closely-related bat Lyssavirus, but it doesn't seem to affect dogs and cats in any significant way, just unfortunate unvaccinated people who happen to grasp hold of a bat and get bitten. Consequently, I have had to read many up-to-date veterinary texts to bring you this information. I hope you enjoyed it and got something out of it.
Kind regards, Dr. O'Meara. BVSc (Hons).
References and Suggested Readings:
1) Field H, Ross T, Emerging Viral Diseases of Bats. In Wildlife in Australia:
Healthcare and Management, Sydney, 1999, Post Graduate Foundation in Veterinary Science, University
of Sydney.
2) Prevention of Infectious Diseases. In Nelson RW, Couto CG, editors: Small Animal Internal Medicine, Sydney, 1998, Mosby Inc.
3) Encephalitis, Myelitis and Meningitis. In Nelson RW, Couto CG, editors: Small Animal Internal Medicine, Sydney, 1998, Mosby Inc.
4) Disorders of the Peripheral Nerves and the Neuromuscular Junction. In Nelson RW, Couto CG, editors: Small Animal Internal Medicine, Sydney, 1998, Mosby Inc.
5) Laboratory Diagnosis of Infectious Diseases. In Nelson RW, Couto CG, editors: Small Animal Internal Medicine, Sydney, 1998, Mosby Inc.
6) Greene CE, Immunoprophylaxis. In Greene CE, editor: Infectious Diseases of the Dog and Cat, St. Louis, 2006, Saunders Elsevier.
7) Greene CE, Rupprecht CE, Rabies and Other Lyssavirus Infections. In Greene CE, editor: Infectious Diseases of the Dog and Cat, St. Louis, 2006, Saunders Elsevier.
8) Greene CE, Environmental Factors in Infectious Disease. In Greene CE, editor: Infectious Diseases of the Dog and Cat, St. Louis, 2006, Saunders Elsevier.
9) Hoskins JD, Canine Viral Diseases. In Ettinger SJ, Feldman EC, editors: Textbook of Veterinary
Internal Medicine, Sydney, 2000, WB Saunders Company.
10) Fenner WR, Diseases of the Brain. In Ettinger SJ, Feldman EC, editors: Textbook of Veterinary
Internal Medicine, Sydney, 2000, WB Saunders Company.
11) Wolf AM, Other Feline Viral Diseases. In Ettinger SJ, Feldman EC, editors: Textbook of Veterinary
Internal Medicine, Sydney, 2000, WB Saunders Company.
12) Groves MG, Harrington KS, Taboada J Frequently Asked Questions About Zoonoses. In Ettinger SJ, Feldman EC, editors: Textbook of Veterinary
Internal Medicine, Sydney, 2000, WB Saunders Company.
13) General Characteristics and Classification of Viruses. In Carter GR, Chengappa MM, Roberts AW editors: Essentials of Veterinary Microbiology, USA, 1995, Williams and Wilkins.
14) Viral Infections of Dogs. In Carter GR, Chengappa MM, Roberts AW editors: Essentials of Veterinary Microbiology, USA, 1995, Williams and Wilkins.
15) Hunt R, RNA Virus Replication Strategies. Hunt R, editor: Microbiology and Immunology Online - http://pathmicro.med.sc.edu/mhunt/RNA-HO.htm, University of South Carolina, 2007.
16) Centers for Disease Control and Prevention: http://www.cdc.gov/rabies/
Copyright April 10, 2008, www.pet-informed-veterinary-advice-online.com.
All rights reserved, protected under Australian copyright. No images or graphics on this Pet Informed website may be used without written permission of their owner, Dr. O'Meara.
Please note: the rabies information contained within this page (including the vaccination schedules,
information on post-exposure prophylaxis, information on treatment of animals
and humans that are bitten by rabid animals, information on human rabies, rabies prevention
methods, shipping of animals into and out of rabies zones and all other rabies information provided) are general recommendations only. The information is provided for general educational
purposes only. The information provided is based on published information and recommendations made available from the vaccine companies themselves and relevant veterinary literature
and publications. We can in no way take responsibility for any disease, death or damage to animals, humans or property that might occur as a result of following this information.
Rabies is a deadly disease. If you or your pet has been potentially exposed to the virus (e.g. through a bite or scratch or contact with a bat) then you must immediately
seek medical attention and information from your local health care provider (or vet) and notify the public health authorities about the incident. Likewise, if you are after specific information concerning rabies vaccines, rabies treatment, animal import/export
laws, rabies vaccination laws, rabies diagnostics laws, rabies treatment laws and the like, you are best to ring your local, regional health department.
Any dose rates mentioned on these pages should be confirmed by a vet. Dosing rates for common
drugs are being changed and updated all the time (e.g. as new research comes in and as drug
formulations change) and information here may not remain current for long. What's more, although we try very hard to maintain the accuracy of our information, typos and oversights do occur. Please check with your vet before dosing any pet any medication or drug.